
Журнал «Актуальная инфектология» 4 (5) 2014
Вернуться к номеру
Nature of the Defeat of the Digestive System in Patients with Drug-Resistant Tuberculosis Using 2nd Line Drugs
Авторы: Boiko А.V. — Bukovinian State Medical University, Chernivtsi, Ukraine
Рубрики: Инфекционные заболевания
Разделы: Клинические исследования
Версия для печати
The prevalence and nature of the defeat of the digestive system, depending on the profile of resistance to antituberculosis drugs in patients with drug-resistant pulmonary tuberculosis in the Chernivtsi region, were established. The main adverse reactions caused by various antibacterial agents, which are most common in the region, are determined, and the evaluation of endogenous intoxication severity in these patients has been carried out.
Установлено поширеність та характер ураження органів системи травлення залежно від профілю стійкості до протитуберкульозних препаратів у хворих на хіміорезистентний туберкульоз легень в Чернівецькій області. Визначено основні побічні реакції, викликані тими чи іншими антибактеріальними засобами, що найчастіше зустрічаються в регіоні, а також проведена оцінка тяжкості ендогенної інтоксикації в таких пацієнтів.
Установлены распространенность и характер поражения органов пищеварительной системы в зависимости от профиля устойчивости к противотуберкулезным препаратам у больных химиорезистентным туберкулезом легких в Черновицкой области. Определены основные побочные реакции, вызванные теми или иными антибактериальными средствами, которые наиболее часто встречаются в регионе, а также проведена оценка тяжести эндогенной интоксикации у таких пациентов.
drug-resistant tuberculosis, side effects of antituberculosis drugs, endogenous intoxication.
хіміорезистентний туберкульоз, побічна дія протитуберкульозних препаратів, ендогенна інтоксикація.
химиорезистентный туберкулез, побочное действие противотуберкулезных препаратов, эндогенная интоксикация.
Статья опубликована на с. 42-45
An important factor for increased incidence of tuberculosis (TB) in different countries of the world is the rapid spread of strains of Mycobacterium tuberculosis (MBT) resistant to anti-TB drugs [11]. In Chernivtsi region, as in the whole country, the upward trend in the incidence of multi-resistant tuberculosis is recorded from 4.1 per 100 thousand of population in 2011 to 5.9 in 2012 (grown by 14.3 %, p < 0.05), which determines the severity and urgency of the problem of treating such patients.
Treatment of drug-resistant forms of tuberculosis, characterized by the rapid multiplication of MBT, massive infiltrative-caseous changes in the lungs, numerous destructions of lung tissue, severe intoxication syndrome, causes considerable difficulties.
One of the main reasons for the lack of efficacy of treatment of this group of patients is adverse side effects that arise during combination therapy of anti-TB drugs. They significantly limit the ability of chemotherapy and reduce the effectiveness of treatment of pulmonary tuberculosis in basic indicators — the terms of cessation of bacterial excretion and frequency of cavities closure [12].
Despite the extensive experience of anti-TB drugs usage, the problem of their side effects on a microorganism remains relevant even today. Since the pre-clinical and clinical trials can not reveal the whole spectrum of possible adverse side reactions to drugs, the need for further research and evaluation of unwanted effects to medication and putting them into practice is rather obvious [13].
Recently, numerous research papers in literature have been devoted to the study of endogenous intoxication (EI) in various pathological diseases because EI is one of the most important criteria that determine the severity of the patient’s condition [1, 7–10]. It is proved that EI develops in any pathological condition. Considering the data of many researchers, EI — is the poisoning of the body by intermediate and final products of metabolism, as a result of their accumulation above normal rate due to either increased catabolism or blockade of detoxification systems of the body, with subsequent damage of other organs and body systems.
Indirect criterion of the severity of condition of patients with different pathological processes is endogenous intoxication severity. In the specialized literature the following components of EI are distinguished: microbiological, biochemical and immunological [8]. In the development of EI among biochemical processes much attention is paid to the activation of proteolysis including general enzymatic homeostasis of the organism disorders.
There is a key concept of the EI syndrome: the emergence of a systemic inflammation can be caused by a variety of pathological processes such as tissue destruction, severe tissue hypoxia and others. It is proved that EI significantly affects the quality of life of patients [1, 8, 10]. It was evidenced that the EI in various pathological conditions arises in the same way. Among the sources of EI the main attention is paid to the foci of inflammatory destruction, ischemic tissues, and zones of natural vegetation flora in the body. The degree of tuberculosis inflammation and the destruction processes are largely determined by the intensity of the release of proteolytic enzymes in the affected area [7].
The objective of the scientific work is to determine the degree of activity of specific inflammatory process in different clinical forms of drug–resistant TB based on complex clinical, laboratory, instrumental and X-ray data, and considering the lack of effective treatment of these patients, one of the reasons for which is the malabsorption of drugs in the intestine, to define the prevalence and nature of digestive system lesions, depending on the profile of resistance to anti-TB medication; to identify the main side effects caused by various anti-TB drugs, which are more common in the region and the ways to improve the pharmacological correction of metabolic changes in individual units, depending on the functional state of the digestive system.
The Results of the Research
The object of the study were 112 patients with newly diagnosed pulmonary drug-resistant TB and 22 patients with preserved resistance of Mycobacterium tuberculosis to anti-TB drugs, who were treated in the hospitals of the 1st and 2nd phtisiatric departments of who were treated in hospitals of the 1st and 2nd divisions Chernivtsi Regional Tuberculosis Dispensary and 20 patients with drug-resistant tuberculosis of the Communal City Institution TB Dispensary, whose anti-TB drugs intolerance has been studied during the period of 2012–2013. The diagnostics of TB and determining the degree of activity of specific inflammatory process were applied on the basis of complex clinical, laboratory, radiological and bronchological data. For comparison, 21 healthy volunteers were studied by the same parameters in the control group.
The results obtained have been processed by the conventional methods using Student’s criterion of distinction and applications software package Microsoft Office XP, Statistica 6.0 (StatSoft ™) [4].
The group of patients under examination was divided according to their ages as follows: young people (20 to 45 years old) accounted for 46.3 %, middle-aged individuals (45 to 59 years old) — 39.02 %, senior people (60 to 74) — 7.3%, elderly patients (75 to 89) — 7.3 %.
The average age of patients was 41.9 ± 1.8 years. Men predominated — 31 (72.1 %).
The patients under examination complained mainly of persistent cough with sputum, fever (37.4–38.9 °C), periodic shortness of breath, weight loss, general weakness. 54.9 % of the patients had satisfactory general condition, 36.1 % — moderate one, and only 9 % — severe.
According to the objective research methods the indicators of heart rate, blood pressure and respiratory rate fluctuated within the normal range and subsequently varied depending on the individual tolerance to chemotherapy. During percussion a clear lung sound prevailed, 20.9 % of patients produced a bandbox lung sound (which is a sign of compensatory emphysema) and 16.2 % — a drum-like tympanic sound, because of large cavities. Through auscultatory percussion 83.7 % of patients demonstrated mostly even weakened vesicular breathing, 16.3 % — with bronchial component. 72.1 % of the surveyed patients had variegated moist crepitant rales over the affected areas of the lungs.
In 78.9 % of patients, tuberculosis process was characterized by the presence of multiple destruction (more than two), massive focal, infiltrative and pneumosclerotic changes in both lungs which go beyond one lobe, complaints of breast pain and severe intoxication syndrome (cough, dyspnoea, febrile temperature increase of the number of red blood cells and neutrophil granulocytes, and erythrocyte sedimentation rate).
Allocating by the forms of the disease the largest group of patients with disseminated pulmonary tuberculosis represented 65.1 %. Infiltrative tuberculosis was diagnosed among 34.9 % of patients.
We analyzed the data on the sensitivity of MBT to anti-TB drugs of the first and second line in Chernivtsi region in 112 patients who were treated in the second phthisiatric department of the regional anti-tuberculosis dispensary. It was proved that 60 (53.6 %) patients had multi-resistance, including: 9 (8 %) — to HR, 22 (19.6 %) — to HRS, 20 (17.8 %) — to HRSE, 3 (2.7 %) — to HRE, other 5.4 % of patients demonstrate resistance to the following combinations of drugs: HRSEt — 1.8 % of patients, HRSZ, HRSKmEt, HRSKmECm, HRSEEt — 0.9 % to each combination. In 24 (21.4 %) patients, MBT mono-resistance was diagnosed: 4 (3.6 %) — isoniazid, 5 (4.5 %) — rifampicin, 11 (9.8 %) — streptomycin, 1 (0.9 %) — to ethambutol, 2 (1.8 %) — to ethionamidum, 1 (0.9 %) — to amikacin. MBT polyresistance was diagnosed in 27 (24.1 %) patients. The most common Mycobacterium tuberculosis was resistant to a combination of HS (10.7 % of patients), much less — to HSE and HEt (2.7 % each), to SE — 0.4 % and to HSEEt — 1.8 % of patients to each combination, to HE, HSKmEt, HSEt, SEt — 0.9 % each. Enhanced resistance of Mycobacterium tuberculosis was diagnosed in 0.9 % of patients.
The development of adverse side effects during the full chemotherapy course for patients with drug-resistant tuberculosis occurs mainly in the first weeks of the intensive phase of treatment. Analysis of the rate of frequency of adverse reactions to anti-TB drugs was carried out among 132 patients with drug-resistant tuberculosis who were treated in the second phthisiatric department of Regional Tuberculosis Dispensary and Municipal City Institution TB Dispensary; it amounts for 15.2 % of the whole number of patients. In 8 % of cases they had to completely withdraw from the further use of anti-tuberculosis drugs that cause side effects.
Analyzing the data of clinical, laboratory tests and ultrasound research of the abdominal organs by 20 patients with drug–resistant tuberculosis, it appears that disruption of the digestive system, mainly by the hepato-pancreato-biliary system in the form of diffuse liver changes, sometimes increasing it, as well as signs of cholecystopancreatitis occur in patients with mono-resistance — 41 %, among patients with multi-resistance in 72 % of cases, with poly-resistance — almost 90 % and all the patients with advanced Mycobacterium tuberculosis resistance.
The study of anti-mycobacterial drugs intolerance showed that among the first- and second-line anti-tuberculosis medications most common side effects occur when taking prothionamide — 30 % of patients who complain of nausea, dizziness, abdominal pain, tachycardia, and application of kanamycin — 25 % of patients noticed deterioration of hearing and tinnitus. 10 % of patients while taking levofloxacin noted arthralgia, myalgia, nausea and dizziness. 15 % of patients receiving pyrazinamide, ethambutol and gatifloxacin observed allergic reactions such as skin rashes and itch. Other 15 % experienced gastrointestinal disorders — diarrhea, nausea, vomiting while taking ofloxacin, coxerin and teriz. With 5 % taking closerin an epileptic attack was observed.
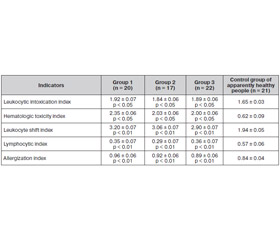
We have selected 59 patients with newly diagnosed destructive pulmonary tuberculosis, which demonstrated changes in hepato-pancreato-biliary system, 20 of which had drug-resistant tuberculosis. They made up the first examination group, the 2nd group consisted of patients with preserved sensitivity of MBT, and the 3d group consisted of 22 patients with pulmonary drug-resistant tuberculosis, who did not reveal disorders of the digestive system. Control group consisted of 21 healthy volunteers (normal subjects).
Most of the examined patients of groups 2 and 3 (57.5 % of cases) revealed moderate intoxication syndrome, as evidenced mainly by febrile body temperature, complaints of general weakness, fatigue, sudden weight loss, lack of appetite, changes in clinical blood: leukocytosis, shift in leukocyte formula, ESR (erythrocyte sedimentation rate) acceleration and expressed catarrhal phenomena in the lungs. X-raying all patients revealed the destruction of the lungs (1 to 3 lesion areas), infiltrative, focal changes of varying prevalence. For a more complete description of the severity of the disease, we determined the number of index indicators — leukocytic intoxication index (LII), hematological intoxication index, leukocyte shift index, lymphocytic index and allergization index. Patients with drug-resistant pulmonary tuberculosis with disorders in the hepato-pancreato-biliary system note an increase in all the index parameters in comparison with other groups and an average of 15 % higher than indicators of healthy people. These patients develop leukocytosis by increasing the relative number of eosinophils and stab neutrophils, there is a significant decrease in the relative number of peripheral blood monocytes.
The reduction of lymphocytic index is a direct sign of the presence of endotoxemia in groups 1–3 in one way or another. Leukopenia and decrease in ESR leads to reduced hematological toxicity index (HTI) and reflects intoxication as a stage of endotoxemia. In the examined groups leukocytosis and increased erythrocyte sedimentation rate and hence increase of HTI were observed, which indicates that there is an intoxication beyond the interstitial space and demonstrates endotoxemia on the peripheral blood level. The biggest divergence of LII and HTI was observed in group 1, indicating a higher severity of endotoxemia (HTI exceeds LII) (Table 1).
/44/44.jpg)
The analysis of the results of the study also suggests that the severity of endogenous intoxication does not depend on the clinical forms of tuberculous processes in the lungs. When comparing the results obtained in the case of infiltrative and disseminated forms no possible difference of indicators was observed.
It should also be noted that toxicity indicators are constantly increasing with the severity of a form of pulmonary tuberculosis. Leukocytic intoxication index is the most sensitive in relation to evaluation of the severity of endogenous intoxication among all the examined groups of patients in our research.
All patients had tests for the indicators of ammonia, urea, creatinine in serum. As a result, it was found that in all cases the levels of ammonia, urea and creatinine in the serum of patients did not exceed the control parameters. The processes that occur during the decay of the lung tissue do not lead to significant changes in these indicators. Perhaps the ammonia is neutralized in the liver with sufficient intensity and its level in serum is not increased. In the absence of renal disease patients with pulmonary tuberculosis do not accumulate ammonia, urea and creatinine in their blood. Namely, the patients have adequate metabolic activity of the liver and excretory renal function in these cases. The phenomenon of endogenous intoxication in pulmonary tuberculosis is not accompanied by the accumulation of low molecular weight products of protein catabolism, such as ammonia, urea and creatinine.
Conclusions
1. Among patients with drug-resistant tuberculosis in Chernivtsi region the most frequent is multi-resistance (resistance mainly to combinations of drugs — HRS and HRSE), MBT resistance to HS and streptomycin. Therefore, in order to reduce the prevalence of drug-resistant TB one should carefully follow the new standards of anti-mycobacterial therapy and improve medication management in the administrative areas, providing supply of medicines and their efficient use.
2. The incidence of adverse reactions to anti-TB drugs is 15.2 % of the general number of patients. Hepato-pancreato-biliary system disorders occur in 41 % of patients with mono-resistance, 72 % — with multi-resistance, almost 90 % — with poly-resistance and all patients with advanced resistance of Mycobacterium tuberculosis.
3. In the absence of renal disease patients with pulmonary drug-resistant tuberculosis do not accumulate ammonia, urea and creatine in blood. The phenomenon of endogenous intoxication is not accompanied by the accumulation of low molecular weight products of protein catabolism.
4. Excessively severe acute phase mobilization of body’s defenses is accompanied by depletion of detoxification reserves, which may cause TB patients to develop a number of negative effects — anemia, hypercoagulability syndrome, malabsorption syndrome, etc., which require appropriate adjustment of treatment programmes. Transfer of patients to the injection treatment regimen of anti-TB drugs enables a 100% control of chemotherapy, provides 100% bioavailability of medicine and reduces the toxic effect potentiating the primary drug, improves the efficiency and shortens the duration of treatment, and also has a pharmacoeconomical effect while treating drug-resistant tuberculosis.
1. Андрейчин М.А., Бех М.Д., Дем’яненко В.В., Ничик А.З., Ничик Н.А. Методи дослідження ендогенної інтоксикації організму: Методичні рекомендації. — К., 1998. — 33 с.
2. Бойчук Т.М. Медико-соціальні проблеми, досягнення та перспективи розвитку фтизіатрії на сучасному етапі / [Бойчук Т.М., Тодоріко Л.Д., Бойко А.В., Сем’янів І.О.] // Укр. терапевт. журн. — 2013. — № 2. — С. 109–115.
3. Борисов С.Е. Клинико–морфологическая диагностика хронических воспалительных заболеваний легких / [Борисов С.Е., Соловьева И.П., Купавцева Е.А., Гончарова Е.В.] // Проблемы туберкулеза и болезней легких. — 2003. — № 11. — С. 42–55.
4. Боровиков В. Statistica. Искусство анализа данных на компьютере: Для профессионалов. — 2–е изд. — М.: Питер, 2003. — 688 с.
5. Гусак В.К. Оценка тяжести эндогенной интоксикации и выбор метода детоксикационной терапии у обожженных по данным лейкоцитограммы и биохимического мониторинга / [Гусак В.К., Фисталь Э.Ц., Сперанский И.И. и др.] // Клин. лаб. диагностика. — 2000. — № 10. — С. 36.
6. Гриппи М.А. Патофизиология легких / Гриппи М.А. — М.: Бином; Х.: МТК–книга, 2005. — 304 с.
7. Дубинина Е.Е. Окислительная модификация протеинов, ее роль при патологических состояниях / Дубинина Е.Е., Пустыгина А.В. // Укр. біохім. журн. — 2008. — № 6. — С. 5–18.
8. Дунтау А.П. Механизмы эндотоксикоза при туберкулезе легких / А.П. Дунтау, А.В. Ефремов, В.В. Бакаев // Пробл. туберкулеза. — 2000. — № 1. — С. 37–39.
9. Инсанов А.Б. Оценка степени эндотоксикоза при туберкулезе легких / Инсанов А.Б. // Материалы 7-го съезда фтизиатров России, 2003.
10. Островский В.К. Показатели крови и лейкоцитарного индекса интоксикации в оценке тяжести и определении прогноза при воспалительных, гнойных и гнойно-деструктивных заболеваниях / [Островский В.К., Мащенко А.В., Янголенко Д.В., Макаров С.В.] // Клин. лаб. диагностика. — 2006. — № 6. — С. 50–53.
11. Наказ МОЗ України від 21.12.2012 № 1091 «Уніфікований клінічний протокол первинної, вторинної (спеціалізованої) та третинної медичної допомоги. Туберкульоз».
12. Неблагоприятные воздействия полихимиотерапии при туберкулезе и некоторые пути их устранения [Електронний ресурс] / Инструкция по применению. Режим доступу: http://s-laboratory.narod.ru/stud/instr.doc
13. Побочные эффекты противотуберкулезных препаратов [Електронний ресурс]. Режим доступу: http://www.sitedf.ru/lechenie/pobochnieEffecti
14. Противотуберкулезные препараты [Електронний ресурс]. Режим доступу: http://www.paco.net/~tuberculos/book/b09.htm