Introduction
These days throughout the world, the global issues are such diseases as chemoresistant tuberculosis (CRTB) and human immunodeficiency virus (HIV), which greatly complicate each other in combined course. At the same time, tuberculosis as an opportunistic disease is one of the main causes of death in HIV-positive patients [1]. Having analyzed the literature data, we found that the course of pregnancy in patients with drug-susceptible tuberculosis/HIV co-infection is sufficiently covered today. However, there are only a few works that highlight this issue in patients with CRTB/HIV co-infection, which is characterized by a more complex course and complications.
So, N. Jana et al. [2] indicated that tuberculosis/HIV co-infection is a “lethal combination” and an independent risk factor for maternal mortality. The authors found the management of pregnancy in such patients challenging, since treatment required co-administration of antituberculosis and antiretroviral drugs. But such therapy caused a large number of adverse drug reactions.
A. Gupta et al. [3, 4] in their studies have found a high prevalence of postpartum tuberculosis among HIV-positive women. It has been shown that tuberculosis/HIV co-infection causes a 2.2-fold increase in maternal mortality and a 3.4-fold — in neonatal mortality rate, intrauterine growth retardation and low birth weight. It further stated that newborns from HIV-positive mothers develop tuberculosis during the first year of life that was an adverse factor and cause of death.
T.G. Gaborets [1] pointed that a pregnancy should not be maintained in HIV-infected women diagnosed with active tuberculosis because of a high risk of obstetric and perinatal complications. In a woman with post-tuberculosis sequelae, pregnancy could be maintained under the supervision of a team of experts that includes physiatrist, gynecologist and infectious disease specialist.
A.V. Nesterenko et al. [5] described the case of tuberculosis diagnosed in HIV-positive pregnant woman at the early stages of pregnancy. It was their clinical follow-up, which showed that the following are preconditions for the birth of a healthy baby to such mother: diagnosis of a specific process at the early stage of gestation, early and adequate antituberculosis chemotherapy combined with antiretroviral therapy, adherence to treatment.
Following a meta-analysis, S. Sobhy et al. [6] found that active tuberculosis in pregnant women is associated with unfavorable maternal and perinatal outcomes underscoring the findings of A. Gupta et al. [3, 4]. In their study, they also demonstrated that maternal mortality was detected in 50 % of pregnant women with tuberculosis/HIV co-infection.
M. Khan et al. [7] described 3 clinical cases of multidrug-resistant tuberculosis (MRTB)/HIV co-infection in pregnant women. All patients received antituberculosis chemotherapy at the time of MRTB diagnosis. The authors indicated that spontaneous abortion was in 1 patient, preterm delivery before gestational week 34 — in 1 patient and 2 newborns were diagnosed with intrauterine growth retardation.
Data of A.V. Nesterenko study [8] have shown that in pregnant women with tuberculosis/HIV co-infection, a specific disease is characterized by the following definite features: the prevalence of disseminated destructive and sputum smear-positive pulmonary tuberculosis as well as the high incidence of MRTB diagnosis (70 %). The author has stated that severe immunosuppression in pregnant women related to HIV and chemoresistance of Mycobacterium tuberculosis (MBT) is correlated with adverse child and maternal outcomes. It has also been found that reliable predictors of ineffective tuberculosis treatment in such patients are: pulmonary tissue destruction, smear-positive tuberculosis, MRTB and tuberculosis progression after pregnancy. It was recommended to administrate an adequate therapy in this case to early correct side effects of antituberculosis drugs. In parallel, the author has pointed that tuberculosis/HIV co-infection is not an indication for induced termination of pregnancy, but the latter should be elective, according to obstetric and general-somatic indications and before gestational week 12.
Objective: to update the literature data with the clinical features of CRTB/HIV co-infection course in pregnant women based on case reports.
Materials and methods
Two own clinical cases of CRTB/HIV co-infection course in pregnant women were described. They received inpatient treatment at the department of pulmonary tuberculosis no. 3 (clinical site of phthisiology and pulmonology department of Zaporizhzhia State Medical University at the Municipal Institution “Zaporizhzhia Regional Tuberculosis Clinical Dispensary” (ZRTBCD)).
Clinical case presentation
Patient 1
A 38-year-old woman G. had no past history of tuberculosis. Preventive fluorographic examination was irregular. Two years ago she had a close contact with a man suffered from tuberculosis, although she did not present any pathological changes as a contact during phthisiological examination. At the same time, the patient’s husband received HIV care by infectionist (B20.0) for a long time. He developed tuberculous pleurisy in this context two years ago, and pleural fluid analysis revealed MBT resistant to isoniazid, rifampicin, streptomycin, ethambutol, and ethionamide. The man had a stroke that caused the death two months after the diagnosis of tuberculosis. For 2 years, phthisiologist repeatedly referred the patient to undergo prophylactic fluorographic examination, but she never responded to requests.
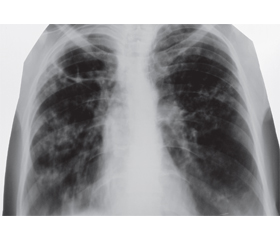
And 3 days before hospital admission to ZRTBCD, the patient complaining of fever and dyspnea visited a general practitioner. As a result, she was hospitalized to the Central District Hospital at the place of residence. After further examination, HIV test was positive and plain chest radiograph showed the following changes (Fig. 1): in both lung fields, predominantly in the middle and basal sections, there was an enhanced interstitial component and small-focal dissemination; both lung hila were infiltrated and poorly structured; sinuses were free; the right hemidiaphragm was deformed due to adhesion.
The patient’s general condition significantly deteriorated. An electrocardiogram showed signs of myocardial hypoxia of the anteroseptal zone.
Clinical blood analysis was as follows: hemoglobin — 88 g/l, red blood cells — 3.5 × 1012/l, leukocytes — 6.2 × 109/l, erythrocyte sedimentation rate — 77 mm/h, banded — 24 %, segmented — 56 %, lymphocytes — 17 %, monocytes — 2 %, eosinophils — 1 %.
Clinical urine analysis: specific gravity — 1017, reaction — acid, protein — 0.297 g/l, erythrocytes — 25–30 per high power field (HPF), renal epithelium — 0–1–2 per HPF, hyaline casts — 2–4 per HPF, granular casts — 2–3 per HPF.
After consulting gynecologist, pregnancy was diagnosed, 32 weeks of gestation.
At the same time, the patient’s state deteriorated cri–tically.
A multidisciplinary team including infectious disease specialist, phthisiologist and gynecologist decided to transfer the patient to the department of anesthesiology and intensive care of ZRTBCD by resuscitation team.
At ZRTBCD, a multidisciplinary team including professors (obstetrician-gynecologist and phthisiologist), regional obstetrician-gynecologist and deputy chief doctor concluded:
1. Patient was newly diagnosed with tuberculosis, disseminated pulmonary tuberculosis, destruction (–), MBT 0. B20.0, IV clinical stage, oropharyngeal and vaginal candidiasis, chronic anemia. Gravida 6 at 32 weeks, para 3, breech presentation, threatened preterm labor.
2. Antituberculosis therapy must be prescribed according to category 1 regimen: isoniazid, rifampicin, pyrazinamide, ethambutol with intensive medical care.
3. Transfer the patient to the Regional Birthing Centre (RBC) in case of labor.
4. Regular monitoring by infectious disease specialist, phthisiologist, gynecologist and anesthetist.
The patient was further diagnosed. She was MTB- and pneumocyst sputum smear-negative. Her HIV antibody test was positive (+), the number of CD4 lymphocytes — 21 cells, viral load — 341820 RNA copies/ml. Taking into account the clinical findings and according to the clinical protocol [9], infectious disease specialist prescribed antiretroviral therapy (ART) for 2 weeks after the beginning of antituberculosis treatment.
Ultrasound showed 32 weeks of pregnancy, fetal heart rate was 150 bpm.
On the fourth day of admission to ZRTBCD, the patient’s clinical condition remained extremely severe and laboratory tests (complete blood count, clinical urine analysis) did not improve. Ultrasound image revealed no detectable fetal heart rate. Gynecologist diagnosed intrauterine fetal demise.
The patient was immediately transferred to RBC: a dead female fetus was delivered. The next day the patient was transferred to the department of anesthesiology and intensive care of ZRTBCD for comprehensive intensive care (antituberculosis, pathogenetic, symptomatic, haemostatic, non-specific antibiotic therapy, etc.) and was supervised by infectious disease specialist, phthisiologist, gynecologist and anesthetist.
Given the patient had a close contact with MRTB husband, she was presented to MRTB expert panel. The patient was graded to category 4 in terms of the risk of MRTB and prescribed the treatment based on the data of her husband’s MBT drug resistance.
However, the general condition of the woman seriously worsened with toxic encephalopathy progression. The patient with suspected meningocephalitis was presented to a multidisciplinary team including infectious disease specialist, clinical neurologist and anesthetist.
The lumbar puncture was performed with cerebrospinal fluid test showing the following parameters: protein — 0.66 g/l, Nonne-Apelt test (+), Pandy’s reaction (++), white blood cell count — 7 cells (lymphocytes), glucose — 2 mmol/l, chlorides — 92.9 mmol/l, MBT and cryptococci were not detected.
Fibrobronchoscopy revealed infiltrative ulcerative tuberculosis of the trachea. Bronchial aspirate test by bacterioscopical method was negative for MBT, atypical cells and pneumocysts.
Three days after the transfer from RBC, despite the comprehensive intensive care, the patient’s general condition deteriorated with increase in signs of multiple organ failure.
All indicators of coagulation profile were increased: fibrin — 17 g, fibrinogen — 377 g, recalcification time — 132 s, prothrombin index — 68.4 s, hematocrit — 22/78 %.
Ultrasound revealed signs of intestinal obstruction and a small amount of free fluid in the pelvic cavity.
Obstetrician-gynecologist consultation: postpartum day 3, intestinal paresis, toxic anemia, thrombocytopenia, toxic encephalopathy.
Surgeon consultation: dynamic intestinal obstruction and intestinal perforation could not be ruled out; an abdominal surgeon consultation was recommended.
Abdominal surgeon advisory opinion: laparoscopy was recommended to rule out a hollow viscus perforation.
On day 4, a multidisciplinary team including infectious disease specialists, phthisiologists, gynecologists, surgeons and anesthesiologist concluded: taking into account signs of peritonitis and suspected intestinal perforation, the patient had to be transferred to the surgical department of the Regional Clinical Hospital.
Patient’s diagnosis upon admission to the Regional Clinical Hospital: pulmonary disseminated MRTB. Destruction (–). MBT (+) M (+). Infiltrative ulcerative extrapulmonary tuberculosis of trachea and intestine. Category 4 (newly diagnosed extrapulmonary tuberculosis). B20, VІ clinical stage, polyorganic insufficiency, oropharyngeal candidiasis, chronic anemia, toxic encephalopathy. Intestinal perforation, peritonitis.
As can be seen in the first case, the patient’s condition severity and rapid disease progression were caused by tuberculosis process spreading due to severe immunodeficiency, which resulted in intrauterine fetal demise (32 weeks), multiple organ failure, intestinal perforation and peritonitis.
Patient 2
A 34-year-old woman Sh. was diagnosed with HIV 8 years ago. The ART course was prescribed, but she took it irregularly. Tuberculosis was newly diagnosed 7 years ago. As a result of the antituberculosis treatment, she was graded to the category 5.1 with minimal post-tuberculosis sequelae.
Recurrent tuberculosis was diagnosed in 5 years. Drug sensitivity test determined MBT resistance to isoniazid, rifampicin, streptomycin following 5 months of treatment. As a result, the patient was diagnosed with pulmonary MRTB of the right upper lobe (infiltrative). Destruction (+), MBT (+) M (+) MG (0), culture (+), resistance I (isoniazid, rifampicin, streptomycin). Category 4 (recurrent tuberculosis). В20.0, VІ clinical stage (CD4 lymphocyte count — 486 cells, viral load — 61757 RNA copies/ml).
The patient was sputum smear-positive (++) on day 240 of MRTB therapy. As a result, a non-response was identified and a repeated course of antituberculosis therapy was administrated.
The patient was back to be sputum smear-positive (+++) on day 300. At the same time, she presented the negative radiological dynamics: 2 cavities of destruction formed in the upper lobe of the right lung with a size of 6.0 × 4.0 cm and 4.0 × 3.0 cm. Surgical treatment was offered repeatedly to the patient, but she refused it.
Thus, the patient received 2 courses of antituberculosis therapy with non-response to treatment, and she interrupted the third course herself. There was no sputum culture conversion. Based on this, according to the clinical protocol [9], it was decided that the patient needed a palliative care.
A year and a half later, the patient consulted phthisiatrist at the district antituberculosis dispensary complaining of weakness, dyspnea, productive cough and spitting up blood. She was sputum smear-positive (MTB +++). Chest X-ray demonstrated bilateral focal infiltrations of all lung fields, predominantly on the right side, with small destructive lesions, and in the right upper lobe — a cavity with destruction, 8.0 cm in diameter, surrounded by fibrosis; diaphragm was deformed due to adhesions; the dynamics was negative caused by an increase in the number of focal infiltrations including on the left side and an increase in the cavity size (Fig. 2).
/61.jpg)
The patient was hospitalized with diagnosis of MRTB of the right upper lobe of the lung (fibrous-cavernous), dissemination phase. Destruction (+), MBT (+) М (+) МG (0) К (+), resistance I (isoniazid, rifampicin, streptomycin, ethambutol), resistance 2 (ethionamide). Category 4. B20.0, VІ clinical stage, severe immunosuppression. Palliative treatment.
The number of CD4 lymphocytes was 156 cells, the viral load — 116708 RNA copies/ml. ART was administrated.
Two months later, the patient told that she was pregnant. After consulting a gynecologist, she was diagnosed with pregnancy, 16 weeks of gestation.
The pelvic organ transabdominal ultrasound was performed: singleton pregnancy, detectable fetal heart rate. Conclusion: ultrasound signs of pregnancy, 16–17 weeks of gestation.
Conclusion of hepatobiliary and urinary system ultrasound: signs of enlargement and diffuse changes of the liver and pancreas, gallbladder congestion, right-side nephroptosis, bilateral diffuse changes of renal parenchyma, typical signs of HIV infection.
Taking into account medical indications (MRTB, HIV infection) and the possible development of complications (tuberculosis progression, development of spontaneous pneumothorax, hemoptysis, tuberculosis and HIV infection transmission to the fetus), the patient was requested to terminate pregnancy. However, she refused and was determined to give birth.
Therefore, for the provision of professional delivery care services, anti-MRTB therapy was administrated again taking into account the results of drug sensitivity test. The patient was hospitalized to ZRTBCD with the subsequent operative delivery at RBC.
She was consulted at RBC. It was found that the patient gave birth 2 times, abortions — 0. Her children were taken off a regular medical check-up due to negative HIV antibody test results. The result of vaginal discharge microscopy: leukocytes — single in the HPF, flora — cocci, gonococci, trichomonads and yeast fungi were not detected. The cervical cytology smear — no atypical cells were detected. The result of colposcopy: the cervix was lined with stratified squamous epithelium, squamocolumnar junction was fully visible; subepithelial vessels were visualized; cervical appearance after application of acetic acid was adequate, Schiller’s test was positive.
Obstetrician-gynecologist recommendations for the further management of pregnancy and childbirth at RBC:
1. Continue the treatment for MRTB and HIV infection at ZRTBCD with adherence to both therapies under control. Social support. Hemostimulating therapy. To test HIV drug resistance.
2. Childbirth at RBC — planned elective caesarian section. Voluntary intraoperative sterilization with the patient’s consent. Vaginal births would be possible with an indicator of viral load < 50 copies of HIV RNA at 38 weeks of gestation.
3. Preventive ART to a newborn (with an indicator of viral load > 50 copies of HIV RNA at 36 weeks of gestation). Child examination on HIV pro-viral DNA (dried blood spot test) within 48–72 hours after birth. Artificial feeding of newborn. Inhibition of lactation.
However, the patient’s general condition critically deteriorated: there was an increase in symptoms of intoxication and pulmonary insufficiency (ventilatory failure, degree 3 of severity), hemoptysis also increased. The patient agreed to terminate the pregnancy at the 20th week of gestation, which was performed at RBC.
Thus, in the second case, the patient did not adhere to treatment of both tuberculosis and HIV infection that was associated with a specific process rapid progression, reported to be life-threatening and was the cause of elective abortion at 20 weeks of gestation.
Conclusions
The presented clinical cases demonstrate the complexity and difficulties in management of CRTB/HIV co-infection in pregnant women due to non-adherence to treatment, rapid diseases progression (tuberculosis process spreading, worsening of immunodeficiency) constituting a life-threatening situation for mothers and increasing perinatal mortality rate.
Conflicts of interests. Authors declare the absence of any conflicts of interests and their own financial interest that might be construed to influence the results or interpretation of their manuscript.
Information about the contribution of each participant
O.M. Raznatovska — concept and design of the study, critical review of the article, its final approval, writing the text; T.A. Grekova — writing the text; A.V. Fedorets — collecting and processing the materials, analysis and interpretation of data obtained; A.I. Pyrog — collecting and processing the materials, analysis and interpretation of data obtained; K.P. Khokhlova — collecting and processing the materials, analysis and interpretation of data obtained.

/59.jpg)
/61.jpg)