Вступ
Стабільність і конгруентність є важливими передумовами ефективного функціонування ліктьового суглоба. Ліктьовий суглоб є одним з найбільш рухливих суглобів тіла і відіграє велику роль у точному позиціонуванні верхньої кінцівки в просторі й забезпеченні координованих рухів кисті.
Середній нормальний діапазон рухів у ліктьовому суглобі становить від 0° до 135° — від повного розгинання передпліччя до гострого кута згинання. Але індивідуальні варіанти рухів можуть відрізнятися. Променево-ліктьовий суглоб завдяки ротації променевої кістки забезпечує просупінаційні рухи до 160°. Мінімальний діапазон руху для необмеженого використання руки в повсякденній діяльності визначається як 0–30–130° (за 0-прохідним методом) і мінімум 50–0–50° просупінації передпліччя.
Ліктьовий суглоб дуже вразливий і схильний до посттравматичного й післяопераційного обмеження рухів. Це пов’язано з нерегулярною формою і високою конгруентністю суглобових поверхонь, необхідних для стабільності й здатності витримувати значні навантаження, що виникають завдяки довгому плечу важеля, утвореного передпліччям. Скелетна анатомія плечо-ліктьового суглоба в нормальних умовах дозволяє практично тільки одну площину рухів, а проксимальний променево-ліктьовий суглоб з комплексом латеральних і колатеральних зв’язок забезпечує просупінаційні рухи. Відносно обмежений суглобовий простір, що забезпечується капсульно-зв’язковим апаратом, і робота м’язів, які працюють як вторинні стабілізатори, роблять ліктьовий суглоб стабільним і здатним витримувати значні навантаження, але, з другого боку, схильним до виникнення контрактур або обмеження рухомості після травми чи операції [1].
Показання до лікування контрактур або обмеження рухів у ліктьовому суглобі відносні й залежать від оцінки пацієнтами функціонального дефіциту. Будь-яке задане обмеження рухливості може мати різні наслідки для різних людей залежно від дискомфорту й бажаного рівня активності. Яке б лікування не було обрано, сильно пошкоджений лікоть ніколи не буде цілком нормальним, і для успішного результату необхідні розумні очікування пацієнта. Виражене обмеження рухливості й стан, що викликає біль і нестабільність суглоба, зазвичай є важливими показниками й показаннями для лікування.
Проведений аналіз сучасної літератури дозволив оцінити можливості консервативних підходів у лікуванні контрактур ліктьового суглоба. Автори стверджують, що за відсутності механічних конфліктів, які викликають обмеження рухливості, таких як неправильне зрощення кісток, вивихи, утворення остеофітів, може бути розглянуто консервативне лікування. Але автори попереджають, що при тривалому існуванні контрактур успіх консервативного лікування часто розчаровує, тому не рекомендують його використовувати, якщо тугорухомість існує понад 6–12 місяців [11]. На ранній стадії може бути корисним шинування, як статичне, так і динамічне [4, 9, 21]. Нехірургічне лікування також включає фізіотерапію, фізичні вправи й пасивну мобілізацію. Безперервні пасивні рухи також пропонувалися деякими дослідниками, але результати виявилися суперечливими, оскільки не було доведено позитивних ефектів, а за твердженнями деяких, застосування цього методу супроводжувалося набряками й проблемами з ліктьовим нервом [3, 7, 10, 15].
Отже, ідеального консервативного метода лікування контрактур ліктьового суглоба немає, а потенціальний внесок нових методів треба доводити.
Ще на початку 60-х років багато дослідників вивчали вплив вібрації на організм людини, у тому числі на суглоби. Але цей інтерес полягав переважно у вивченні негативного впливу вібрації і пов’язаного з ним розвитку професійних захворювань. Десь наприкінці 80-х років оновився інтерес до низькочастотних механічних коливань уже щодо вивчення їх позитивного впливу на організм, у тому числі як терапевтичного методу лікування деяких ортопедичних захворювань [16, 20]. З’явився новий термін — «вібротерапія».
Вібротерапія (лат. vibrare — дрижати, коливатися + грец. therapeia — лікування) — метод лікувального впливу механічними хвилями низької частоти, що здійснюється при безпосередньому контакті з тканинами або тілом хворого. Дія вібротерпії визначається впливом на тканини механічних хвиль низької частоти й вибірковим збудженням вібрацією різних механорецепторів, які приводять до низки фізіологічних змін і саногенетичних ефектів. В основі фізіологічного впливу вібрації на організм лежать механічні, фізико-хімічні й теплові (які проявляються меншою мірою) ефекти. Вираженість відповідних фізіологічних механізмів залежить від інтенсивності й параметрів (частоти, амплітуди) впливу, умов проведення й локалізації [12, 14, 16, 20].
Найбільш важливими ефектами є аналгетичний, трофічний, протизапальний, лімфодренувальний, вазоактивний і тонізуючий. За дією апаратуру для вібротерапії поділяють на пристрої для місцевої вібрації (вібромасаж) і апарати загальної вібрації — для всього тіла.
У частот, які використовують у фізіологічній реабілітації, виділяють такі діапазони:
1) до 16 Гц — інфразвук;
2) 16–20 000 Гц — чутний звук;
3) від 20 000 Гц (20 кГц) до 1000 МГц — ультразвук;
4) понад 1000 МГц — гіперзвук.
Найбільш помітно впливають на тканини організму частоти в діапазоні 10–200 Гц.
Механічні коливання частотою понад 20–50 Гц викликають вибіркове подразнення механорецепторів, судин, вегетативних нервових провідників, що призводить до розширення судин м’язового типу, посилення локального кровотоку й лімфовідтоку, сприяє зниженню м’язового тонусу й активації трофічних процесів у тканинах.
Одним з головних впливів лікувальної дії вібрацій є знеболювальна дія. Механізм знеболюючої дії вібрацій обумовлений адаптацією організму у зв’язку з розвитком у центральній нервовій системі явищ гальмування. Слабкі вібраційні подразнення викликають судинозвужувальний ефект, сильні — розширення судин. При низьких частотах механічних коливань виникає атонія судин, при високочастотних коливаннях (100–200 Гц) — спазм судин. Механічні коливання при певних частотах передаються в центральну нервову систему й реалізуються на периферії у вигляді короткочасних м’язових скорочень.
Вібрація діє по всьому об’єму м’язів, відбувається значне збільшення скорочувальної здатності м’язів, посилюється обмін речовин без накопичення молочної кислоти, що дозволяє швидко відновлювати м’язи після фізичного навантаження, прискорюються процеси репарації після травм м’язів. Вібрація сприяє м’язовій релаксації, посиленню м’язового розтягування, підвищує еластичність зв’язок і сухожилків, збільшує рухливість у суглобово-зв’язковому апараті, нормалізує трофічні процеси, сприяючи повноцінному виробленню синовіальної рідини [2, 5]. Контрактури, які формуються при іммобілізації, відповідають на низькочастотну вібрацію, яка прикладена безпосередньо до ураженого суглоба. Позитивний вплив низькочастотних коливань на збільшення амплітуди рухів у суглобах відмічений багатьма дослідниками, але комплексного дослідження проведено не було.
У даній роботі ми розглядаємо консервативні методи лікування, а саме вплив вібрації і постізометричної релаксації на контрактуру ліктьового суглоба, що виникла внаслідок тривалої іммобілізації після хірургічного втручання, пов’язаного з позасуглобовими переломами плечової, променевої і ліктьової кісток, а також виростка плечової кістки. При всіх травмах не було ушкоджень тканин суглоба.
Мета роботи полягає у вивченні впливу низькочастотної вібрації на зменшення післятравматичної тугорухливості ліктьового суглоба.
Матеріали та методи
Проведено вібротерапію 21 пацієнту з контрактурами ліктьового суглоба, які сформувалися після позасуглобових переломів кісток верхньої кінцівки. Усім пацієнтам виконували хірургічну стабілізацію відламків кісток верхньої кінцівки. Після операції використовували різні засоби фіксації — гіпсову шину, функціональний ортез, апарат Ілізарова. Вік пацієнтів був від 20 до 60 років.
Пацієнти були поділені на 2 групи. І групу — 14 (66,7 %) становили пацієнти, термін обмеження рухливості суглоба в яких становив від 21 до 45 діб. Ці пацієнти малі обмеження рухів у ліктьовому суглобі, тобто післяіммобілізаційні контрактури, які ми оцінювали як контрактури міогенного характеру.
ІІ групу — 7 (33,3 %) становили пацієнти, термін обмеження рухливості ліктьового суглоба яких становив від 90 до 180 діб. Деякі пацієнти цієї групи через складні травми перенесли декілька етапів хірургічного лікування, кілька пацієнтів отримували консервативне лікування — фізіо- і механотерапію. Ці контрактури ми оцінювали як контрактури міо-, артро-, десмогенного характеру.
Пацієнтам обох груп пропонували стандартний курс вібротерапії. Тривалість курсу вібротерапії становила 14–15 сеансів по 10 хв. Вимірювання обсягу рухів (розгинання/згинання) проводили до і після кожної процедури. Частота вібраційного впливу становила 20 Гц. Під час вібраційної процедури пацієнти виконували вправи з елементами постізометричної релаксації (ПІР), треба було за допомогою вільної руки зафіксувати розгинання на 10 с, потім на 10 с розслабити кінцівку і повторити вправи зі згинанням передпліччя. Цикл складався з 10–15 повторів. Між циклами — вільне розташування на віброплатформі (відпочинок). Таких циклів у процедурі було 10–12.
При аналізі результатів вібротерапії оцінювали 1, 2, 5, 10-й і останній день процедур. Через те, що конт-рактури ліктьового суглоба в пацієнтів були різного ступеня вираженості, зміни оцінювали в абсолютних одиницях і відсотках.
Результати
Вібротерапію починали проводити за умови відсутності болю, виражених поверхневих ушкоджень і набряків суглоба. На першому сеансі пацієнту показували необхідні вправи для розробки, обирали зручну позу, висоту посадки й положення ліктьового суглоба на апараті. У більшості пацієнтів вже після першого сеансу спостерігали збільшення обсягу рухів. Результати вібротерапії пацієнтів з контрактурами ліктьового суглоба наведені в табл. 1, 2.
На початку проведення 1-го сеансу вібротерапії в пацієнтів спостерігали обмеження розгинання до 41 ± 8° і згинання — до 108 ± 20° (табл. 1), при цьому загальний обсяг рухів становив у середньому 67 ± 18° (табл. 2). Результати вібраційної розробки ліктьового суглоба помітні вже після першої процедури, розгинання збільшилося в середньому до 35 ± 8°, що становило приріст на 16,4 ± 9,3°, а розгинання збільшилося до 113,8 ± 17,4°, тобто на 7 ± 6 %. Загальне збільшення обсягу рухів після першого сеансу становило 19,2 ± 10,5 % — до 78 ± 17°.
Динаміка збільшення обсягу рухів збереглася, і після другої процедури відмічали збільшення розгинання на 16,0 ± 14,3 % і згинання — на 7,8 ± 4,2 %, збільшення загального обсягу рухів становило 17,5 ± 9,6 %.
Поступове збільшення обсягу рухів у ліктьовому суглобі відбувалося в наступні 5–7 процедур. На 5-ту добу спостереження обсяг розгинання в середньому досяг 29 ± 7°, розгинання — 120 ± 17°, загальний обсяг рухів становив 91 ± 18°. Приріст за процедуру становив у середньому 12,6 ± 12,1 %.
Відмітимо, що в пацієнтів спостерігалась часткова втрата обсягу рухів між процедурами, особливо в перші 5–7 діб (табл. 3). Найбільші втрати обсягу рухів спостерігали на початок 2-ї процедури — 12,1 ± 13,3 %. У подальшому втрата обсягу рухів між процедурами загальмувалась.
Починаючи з 5-ї доби за відсутності дискомфорту під час проведення процедур і після них пацієнтам пропонували збільшити якість та інтенсивність вправ на згинання й розгинання передпліччя з елементами ПІР.
На 10-ту добу вібраційних процедур загальний обсяг рухів у середньому сягав 103 ± 16°, причому втрати обсягу рухів зменшилися.
У пацієнтів другої групи з довгим терміном обмеження рухів у ліктьовому суглобі спостерігалася інша динаміка відновлення рухів.
У табл. 4, 5 наведені результати впливу вібраційного лікування на розробку рухів у ліктьовому суглобі в пацієнтів другої групи.
До початку вібраційних процедур кут розгинання ліктьового суглоба в пацієнтів у середньому становив 58 ± 9°, а згинання — 86 ± 11°, обсяг рухів — 29 ± 19°. Після першої процедури практично в усіх пацієнтів спостерігали незначне, в середньому на 18 ± 7 %, збільшення обсягу рухів. Зміна кутів згинання/розгинання становила до 6 %.
На початок другої процедури спостерігали зменшення досягнутого обсягу рухів (до 14,0 ± 8,2 %) (табл. 6), але після неї отримували його приріст до 28,8 ± 16,6 %, причому як розгинання — на 5,1 ± 2,3 %, так і згинання — на 4,1 ± 2,4 %.
Після 4–5-ї процедури в пацієнтів відмічали гальмування приросту обсягу рухів, тому радили хворим збільшити якість та інтенсивність вправ на згинання і розгинання передпліччя з елементами ПІР, за можливості — з обтяженням до 1,0 кг. У деяких пацієнтів це приводило до відновлення приросту обсягу рухів, у деяких — ні, але повільний приріст тривав.
На відміну від результатів відносно ранніх контрактур, стійкі контрактури гірше піддаються вібраційній розробці. Ми спостерігали значно менший приріст обсягу рухів після процедур, до того ж втрати обсягу рухів між процедурами відбувалися впродовж усього курсу (табл. 6)
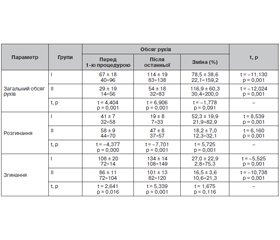
У табл. 7 подані результати вібраційної розробки контрактур пацієнтів І і ІІ груп.
Після проходження процедур вібророзробки ліктьового суглоба (табл. 7) у пацієнтів І групи загальний обсяг рухів досяг у середньому 114 ± 19°, що становило 78,5 ± 38,6 %, у ІІ групі загальний обсяг рухів досяг 54 ± 18°, тобто відбулося збільшення на 116,9 ± ± 60,3 %. Досягнутий обсяг рухів в І групі був статистично значущо (р = 0,001) більший, ніж у ІІ групі. Зміна обсягу рухів в обох групах була статистично значущою (р = 0,001).
Розгинання після останньої процедури в І групі хворих становило 19 ± 8°, згинання — 134 ± 14°, у ІІ групі — 47 ± 8° і 101 ± 13° відповідно, результати в І групі були статистично кращі (р = 0,001), ніж у ІІ групі.
Загальний приріст кута розгинання у хворих І групи становив 52,3 ± 19,9 % від початкового рівня, у хворих ІІ групи — 18,2 ± 7,0 %, приріст кута згинання становив 27,0 ± 22,9 % і 16,5 ± 3,6 % відповідно.
Відмітимо, що в пацієнтів ІІ групи первинний обсяг рухів був значущо меншим, ніж у пацієнтів І групи, а після розробки у хворих ІІ групи не було досягнуто значного збільшення обсягу рухів, навіть до первинних значень обсягу рухів у І групі.
Обговорення
Проведений аналіз літератури показав, що основними консервативними механічними методами лікування іммобілізаційних контрактур є масаж, механорозробка й застосування пасивних або динамічних ортезів. Але, за даними метааналізів, ці методи не приводять до бажаних результатів, особливо при застарілих контрактурах [6, 17, 18].
За даними деяких авторів, останніми роками була доведена ефективність циклічної розробки суглобів щодо загоєння тканин, а також щодо відновлення функції суглобів [8, 13]. Цікавими виявилися дослідження деяких авторів щодо застосування прогресивних вправ з обтяженням для збільшення здатності м’язів генерувати силу [19].
У даному дослідженні для розробки іммобілізаційних контрактур ліктьового суглоба ми поєднали метод низькочастотного локального вібраційного впливу з вправами з елементами постізометричної релаксації. У нашому досвіді це дозволило якщо не повністю відновити обсяг рухів у ліктьовому суглобі, то хоча б зрушити з мертвої точки процеси відновлення.
У процесі дослідження були вироблені деякі принципи проведення вібраційної розробки контрактур суглобів:
1. Вібротерапію починають проводити за відсутності гострих больових відчуттів, виражених пошкоджень шкіри, конструктивних елементів фіксації відламків, які можуть бути пошкоджені при вібрації.
2. Перед початком проведення курсу вібротерапії проводять навчання щодо виконання необхідних вправ (ПІР), обирають зручну позу, висоту посадки й установки кінцівки на вібростенді. Сеанс триває 10 хв. При появі неприємного відчуття або болю сеанс може бути скороченим, але це, за нашими спостереженнями, відбувається в перші 2–3 сеанси.
3. Перед початком і після закінчення кожної процедури проводять вимірювання обсягу рухів.
4. Особливу увагу зміні обсягу рухів слід приділити на 5–7-му сеансі. У цей час приріст рухливості зазвичай уповільнюється. Пацієнтам рекомендують збільшити інтенсивність ПІР.
5. Курс вібраційної розробки триває 14–15 сеансів. За рекомендаціями лікаря курс може бути продовженим.
Проведений аналіз даних вібротерапії показав, що пацієнти, у яких контрактури сформувалися після короткої (до 1,5 місяця) іммобілізації, краще відповідають на вібраційну розробку, приріст розгинання становить близько 50 % від початкового рівня, обсяг згинальних рухів збільшується до 30 %.
У пацієнтів з контрактурами після тривалої іммобілізації понад 3 місяці розробка йде дуже повільно, досягнуті обсяги рухів дуже далекі від нормальних. Приріст згинання/розгинання в ліктьовому суглобі не перевищує 20 %.
Висновки
Низькочастотна локальна вібраційна розробка рухів у ліктьовому суглобі й розтягувальні вправи з елементами постізометричної релаксації є прогресивним методом розробки іммобілізаційних контрактур, у тому числі застарілих. Дані процедури в більшості випадків не приводять до нормалізації обсягу рухів, але дають позитивний поштовх до подальшого відновлення класичними методами механо- і фізіотерапії. Низькочастотна вібрація є тим механізмом, який запускає процеси відновлення, тому доцільно починати її якнайшвидше після припинення лікувальної іммобілізації.
Дана робота є першою в комплексному дослідженні впливу вібрації низької частоти на відновлення іммобілізаційних контрактур.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів і власної фінансової зацікавленості при підготовці даної статті.
Отримано/Received 30.06.2022
Рецензовано/Revised 07.07.2022
Прийнято до друку/Accepted 15.07.2022
Список литературы
1. Adolfsson L. Post-traumatic stiff elbow. EFORT Open Rev. 2018 May 21. 3(5). 210-216. doi: 10.1302/2058-5241.3.170062.
2. Bidonde J., Busch A.J., Spuy I., Tupper S., Kim S.Y., Boden C. Whole body vibration exercise training for fibromyalgia. Cochrane Database Syst. Rev. 2017. doi: 10.1002/14651858.CD011755.pub2.
3. Carpenter C.V., Amirfeyz R. Continuous passive motion following elbow arthrolysis. J. Hand Surg. Am. 2014. 39. 350-352.
4. Doornberg J.N., Ring D., Jupiter J.B. Static progressive splinting for posttraumatic elbow stiffness. J. Orthop. Trauma. 2006. 20. 400-404.
5. Games K.E., Sefton J.E.M., Wilson A.E. Whole-Body Vibration and Blood Flow and Muscle Oxygenation: A Meta-Ana-lysis. J. Athl. Train. 2015. 50(5). 542-549. doi: 10.4085/1062-6050-50.2.09
6. Harvey L.A., Katalinic O.M., Herbert R.D., Moseley A.M., Lannin N.A., Schurr K. Stretch for the treatment and prevention of contractures. Cochrane Database of Systematic Reviews. 2017, Issue 1. Art. No.: CD007455. DOI: 10.1002/14651858.CD007455.pub3
7. Higgs Z.C., Danks B.A., Sibinski M., Rymaszewski L.A. Outcomes of open arthrolysis of the elbow without post-operative passive stretching. J. Bone Joint Surg. [Br.] 2012. 94-B. 348-352. [PubMed] [Google Scholar]
8. Khan K.M., Scott A. Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. Br. J. Sports Med. 2009 Apr. 43(4). 247-52. doi: 10.1136/bjsm.2008.054239.
9. Lindenhovius A.L., Doornberg J.N., Brouwer K.M., et al. A prospective randomized controlled trial of dynamic versus static progressive elbow splinting for posttraumatic elbow stiffness. J. Bone Joint Surg. [Am.] 2012. 94-A. 694-700.
10. Lindenhovius A.L., van de Luijtgaarden K., Ring D., Jupiter J. Open elbow contracture release: postoperative management with and without continuous passive motion. J. Hand Surg. Am. 2009. 34. 858-865.
11. Mellema J.J., Lindenhovius A.L., Jupiter J.B. The posttraumatic stiff elbow: an update. Curr. Rev. Musculoskelet. Med. 2016. 9. 190-198
12. Nagai T., Bates N.A., Hewett T.E., Schilaty N.D. Effects of Localized Vibration on Knee Joint Position Sense in Individuals with Anterior Cruciate Ligament Reconstruction. Clin. Biomech (Bristol, Avon). 2018. 55. 40-44. doi: 10.1016/j.clinbiomech.2018.04.011
13. Ng J.L., Kersh M.E., Kilbreath S., Knothe Tate M. Establishing the Basis for Mechanobiology-Based Physical Therapy Protocols to Potentiate Cellular Healing and Tissue Regeneration. Front. Physiol. 2017. 8. 303. doi: 10.3389/fphys.2017.00303..
14. Novotny S.A., Eckhoff M.D., Eby B.C., Call J.A., Nuckley D., Lowe D.A. Musculoskeletal response of dystrophic mice to short term, low intensity, high frequency vibration. J. Musculoskelet. Neuronal Interact. Author manuscript; available in PMC 2020 Mar 14.
15. O’Driscoll S.W., Giori N.J. Continuous passive motion (CPM): theory and principles of clinical application. J. Rehabil. Res. Dev. 2000. 37. 179-188.
16. Peelukhana S.V., Goenka S., Kim B., Kim J., Bhattacharya A., Stringer K.F., Banerjee R.K. Effect of higher frequency components and duration of vibration on bone tissue alterations in the rat-tail model. Ind. Health. 2015. 53(3). 245-259. doi: 10.2486/indhealth.ih-2014-0117
17. Prabhu R.K.R., Swaminathan N., Harvey L.A. Passive movements for the treatment and prevention of contractures. Cochrane Database of Systematic Reviews 2013, Issue 12. Art. No.: CD009331. DOI: 10.1002/14651858.CD009331.pub2
18. Skalsky A.J., McDonald C.M. Prevention and management of limb contractures in neuromuscular diseases. Phys. Med. Rehabil. Clin. N. Am. 2012 Aug. 23(3). 675-87. doi: 10.1016/j.pmr.2012.06.009.
19. Taylor N.F., Dodd K.J., Damiano D.L. Progressive resistance exercise in physical therapy: a summary of systematic reviews. Phys. Ther. 2005 Nov. 85(11). 1208-23. PMID: 16253049.
20. Tseng S.-C., Shields R.K. Limb segment load inhibits the recovery of soleus h-reflex after segmental vibration in humans. J. Mot. Behav. 2018. 50(6). 631-642. doi: 10.1080/00222895.2017.1394259
21. Veltman E.S., Doornberg J.N., Eygendaal D., van den Bekerom M.P. Static progressive versus dynamic splinting for posttraumatic elbow stiffness: a systematic review of 232 patients. Arch. Orthop. Trauma Surg. 2015. 135. 613-617.

/53.jpg)
/54.jpg)
/55.jpg)