
Журнал «Боль. Суставы. Позвоночник» Том 12, №4, 2022
Вернуться к номеру
Мінеральна щільність кісткової тканини та інші фактори ризику в дітей та підлітків із низькоенергетичними переломами довгих кісток
Авторы: F.Х. Umarov, Z.М. Matanov
State Institution “Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of the Ministry of Health of the Republic of Uzbekistan”, Tashkent, Republic of Uzbekistan
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
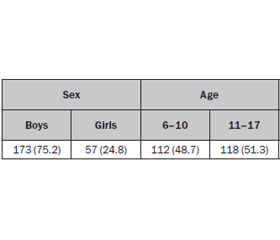
Актуальність. Відзначається збільшення кількості дітей та підлітків зі зниженими віковими темпами накопичення кісткової маси, низьким рівнем мінеральної щільності кісткової тканини (МЩКТ) та переломами. Ця проблема широко висвітлюється в науковій літературі. Мета: оцінити показники МЩКТ у дітей та підлітків із низькоенергетичними переломами довгих кісток і рівень кальцію, фосфору, вітаміну D та лужної фосфатази в сироватці крові. Матеріали та методи. Досліджено індекс маси тіла, показники кісткової денситометрії, рівні вітаміну D, кальцію, фосфору та лужної фосфатази в сироватці крові 230 дітей та підлітків (173 хлопчики та 57 дівчаток) віком від 6 до 17 років, які знаходились на лікуванні з приводу переломів довгих кісток. Результати. Переломи відбувалися переважно в плечовій кістці (41,3 %) та кістках передпліччя (43 %). У 20 % дітей та підлітків із переломом спостерігалися відхилення від нормальних показників індексу маси тіла. Низькі показники МЩКТ у 86 з 230 обстежених виявлено в поперековому відділі хребта, лише в 66 (76,7 %) випадках порушення МЩКТ були наявні в проксимальному відділі стегнової кістки. При оцінці статусу вітаміну D показники були нормальними в 19,3 % дівчаток і 9,2 % хлопчиків. Виявлено зниження рівня кальцію та підвищення лужної фосфатази в сироватці крові. За показниками кореляції МЩКТ та вітаміну D у хлопчиків залежність ознак була статистично значущою в молодшому та старшому шкільному віці, у дівчаток — лише в молодшому шкільному. Установлено прямий зв’язок між низькими показниками МЩКТ та вітаміну D. Висновки. Низькі показники МЩКТ, вітаміну D, порушення фосфорно-кальцієвого обміну й ожиріння в дітей та підлітків можуть бути предикторами перелому.
Background. There are an increasing number of children and adolescents with reduced age-related rate of bone mass accumulation, low bone mineral density (BMD) and low-energy fractures. This problem is widely discussed in the scientific literature. Purpose of the study was to assess the BMD in children and adolescents with low-energy fractures of long bones and to investigate some biochemical parameters of bone metabolism. Materials and methods. Body mass index (BMI), bone densitometry, levels of vitamin D, calcium, phosphorus and alkaline phosphatase in blood serum of 230 children and adolescents with low-energy fractures of long bones, aged 6 to 17 years, who underwent treatment due to the fractures were studied. Results. Fractures occurred predominantly in 41.3 % of the humerus and 43 % of the forearm bones. 20 % of children and adolescents had abnormal BMI values. Low BMD values in 86 of 230 examinees were detected in the lumbar spine, of which only 66 (76.7 %) had BMD abnormalities in the hip. In assessing vitamin D status, 19.3 % of the girls and 9.2 % of the boys had normal vitamin D values. A decrease in calcium level and an increase in alkaline phosphatase in blood serum were found. In terms of BMD and vitamin D status, the dependence of boys was statistically significant in the elementary and high school groups, while in girls it was only in the elementary school group. A direct link between low BMD and vitamin D has been established. Conclusions. Low BMD, vitamin D, impaired calcium-phosphorus metabolism and obesity in children and adolescents may be considered predictors of fracture occurrence.
діти; підлітки; перелом; мінеральна щільність кісткової тканини; вітамін D; лабораторні показники
children; adolescents; fracture; bone mineral density; vitamin D; laboratory indices
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Campos L.M., Liphaus B.L., Silva C.A., Pereira R.M. Osteoporosis in childhood and adolescence. J. Pediatr. (Rio J). 2003 Nov-Dec. 79(6). 481-488 (in Portuguese).
- Ciancia S., van Rijn R.R., Högler W. et al. Osteoporosis in children and adolescents: when to suspect and how to diagnose it. Eur. J. Pediatr. 2022 Jul. 181(7). 2549-2561. doi: 10.1007/s00431-022-04455-2.
- Sakka S.D., Cheung M.S. Management of primary and secondary osteoporosis in children. Ther. Adv. Musculoskelet. Dis. 2020 Nov 2. 12. 1759720X20969262. doi: 10.1177/1759720X20969262.
- Korula S., Titmuss A.T., Biggin A., Munns C.F. A Practical Approach to Children with Recurrent Fractures. Endocr. Dev. 2015. 28. 210-225. doi: 10.1159/000381047.
- Steffey C.L. Pediatric Osteoporosis. Pediatrics in Review. 2019. 40. 259. doi: 10.1542/pir.2017-0277.
- Bishop N., Arundel P., Clark E. et al. Fracture prediction and the definition of osteoporosis in children and adolescents: the ISCD 2013 Pediatric Official Positions. Journal of Clinical Densitometry. 2014. 17. 275-280. doi: 10.1016/j.jocd.2014.01.004.
- World Health Organisation. BMI-for-age (5–19 years). Available from: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age.
- Holick M.F., Binkley N.C., Bischoff-Ferrari H.A. et al.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011 Jul. 96(7). 1911-1930. doi: 10.1210/jc.2011-0385.
- Hightower L. Osteoporosis: pediatric disease with geriatric consequences. Orthopaedic Nurs. 2000. 19(5). 59-62.
- ISCD 2019. Official Positions Pediatric. Available from: https://iscd.org/wp-content/uploads/2021/09/2019-Official-Positions-Pediatric-1.pdf.
- Frolova O.V., Okhapkina N.F., Stenkovaya I.I. et al. Osteopenic disorders in schoolchildren: algorithm of diagnosis and prognostic criteria. Pediatria. International Medical Journal. 2008. (4). 30-36. Available from: http://dspace.nbuv.gov.ua/bitstream/handle/123456789/54122/07-Frolova.pdf?sequence=1.
- Tourilina E.V., Sveshnikov A.А., Astapenkov D.S. The spine mineral density in children and adults. Genius Orthopedics. 2007. 4. 115-119. Available from: https://cyberleninka.ru/article/n/mineralnaya-plotnost-pozvonochnika-u-detey-i-vzroslyh.
- Sarinhoa E.S.C., Melo V.M.P.P. Glucocorticoid-induced bone disease: mechanisms and importance in pediatric practice. Rev. Paul. Pediatr. 2017. 35(2). 207-215. doi: 10.1590/1984-0462;2017/;35;2;00007.
- Shchepliahyna L.A., Kruhlova Y.V., Moyseeva T.Iu. The origins of adult osteoporosis lie in childhood. Treatment and prevention. 2013. 5(1). 6-13. Available from: https://www.lechprof.ru/catalog/article/editorial/the_origins_of_osteoporosis_are_adults_in_children.
- Chiarpenello J. Diagnosis of Osteoporosis in Children. Endocrinol. Metab. Syndr. 2016. 5. 237. doi: 10.4172/2161-1017.1000237.
- Chevalley T., Bonjour J.P., Rietbergen B. et al. Fractures during childhood and adolescence in healthy boys: relation with bone mass, microstructure, and strength. J. Clin. Endocrinol. Metab. 2011. 96. 3134-42. doi: 10.1210/jc.2011-1445.
- Singhal V., Huynh C., Nimmala S. et al. Load-to-strength ratio at the radius is higher in adolescent and young adult females with obesity compared to normal-weight controls. Bone. 2022 Nov. 164. 116515. doi: 10.1016/j.bone.2022.116515.
- Rajakumar K., Fernstrom J.D., Janosky J.E. et al. Vitamin D Insufficiency in Preadolescent African-American Children. Clinical Pediatrics. 2005. 44(88). 683-692. doi: 10.1177/000992280504400.
- Vimalraj S. Alkaline phosphatase: Structure, expression and its function in bone mineralization. Gene. 2020. 754(1448555). doi: 10.1016/j.gene.2020.144855.