
Журнал «Почки» Том 12, №3, 2023
Вернуться к номеру
Кореляція рівнів ліпокаліну, асоційованого з желатиназою нейтрофілів, у сечі як ранній діагностичний маркер гострого ураження нирок у пацієнтів із сепсисом
Авторы: Srija Yadav Kadari, Swarna Deepak Kuragayala, Nagender Devulapally, Sivateja Kuruvada
Apollo Institute of Medical Sciences and Research, Hyderabad, Telangana, India
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
Актуальність. Невідомий точний зв’язок між ліпокаліном, асоційованим із желатиназою нейтрофілів, у сечі (uNGAL) та гострим пошкодженням нирок (ГПН) у реанімаційних умовах, коли популяція є гетерогенною, а етіологія ГПН неясна. Мета: з’ясувати, чи є рівні uNGAL раннім діагностичним маркером ГПН у пацієнтів із сепсисом. Матеріали та методи. Поточне дослідження проведено за участю 86 хворих на сепсис, серед яких було визначено поширеність ГПН. Проаналізовано роль uNGAL у прогнозуванні розвитку ГПН, рівня смертності та тривалості перебування у відділенні інтенсивної терапії. Були розраховані чутливість і специфічність, а площа під кривою робочої характеристики приймача вважалася пороговим рівнем uNGAL, оптимальним щодо виявлення всіх типів ГПН. Результати. Більшість пацієнтів належали до вікової групи 51–60 років, середній вік становив 54,6 року. Більшість хворих (65,11 %) були чоловіками, 26,75 % мали цукровий діабет 2-го типу та гіпертензію. ГПН спостерігалося в 89 % суб’єктів поточного дослідження згідно з визначенням KDIGO. ХХН 1-ї стадії діагностовано в 15,12 % пацієнтів, 2-ї — у 15,12 %, 3-ї стадії — у 4,65 %. Рівень смертності становив 11 %, 89 % пацієнтів були виписані. Середня тривалість перебування хворих із ГПН у реанімації становить 8,9 дня. Існує значний зв’язок між середньою тривалістю перебування у відділенні інтенсивної терапії і наявністю ГПН (p = 0,03). Замісної ниркової терапії потребували 17,4 % (n = 15) пацієнтів. Існує вірогідна різниця в середньому базовому рівні uNGAL в осіб із ГПН та без нього: 149,9 і 73,2 нг/мл відповідно (p = 0,0006). Це вказує на те, що базові рівні uNGAL дозволяють спрогнозувати ГПН. Середнє значення uNGAL у хворих із ГПН становить 356 нг/мл, в осіб без ГПН — 95 нг/мл. Через 48 годин спостерігається дуже значна різниця в середньому рівні uNGAL у пацієнтів із ГПН та без нього (p < 0,0001). При граничному значенні 120 було 69 істинно позитивних, 9 істинно негативних, 0 хибнопозитивних і 8 хибнонегативних випадків. Виходячи з цього, чутливість uNGAL на початковому рівні у виявленні ГПН становить 89,61 %, специфічність — 100 %, а точність — 90,70 %. При граничному значенні 120 було 77 істинно позитивних випадків, 8 істинно негативних випадків, 1 хибнопозитивний випадок і 0 хибнонегативних випадків. З огляду на це чутливість uNGAL через 48 годин становила 100 %, специфічність — 88,89 %, а точність — 98,84 %. Існує вірогідний зв’язок між рівнем uNGAL і тривалістю перебування у відділенні інтенсивної терапії (p = 0,00). Висновки. Аналіз чутливості проводився при пороговому значенні 120 для uNGAL щодо прогнозування ГПН. Таким чином, ми робимо висновок, що uNGAL на момент надходження у відділення інтенсивної терапії є надійним маркером функції нирок у пацієнтів із сепсисом. Існує суттєва кореляція між наявністю ГПН, рівнем uNGAL та тривалістю перебування у відділенні інтенсивної терапії. Ми рекомендуємо не використовувати тільки uNGAL для прогнозування ГПН — його слід поєднувати зі швидкістю клубочкової фільтрації, щоб надійно діагностувати ГПН. Результати дослідження вказують на те, що пацієнти із сепсисом і підвищеним рівнем uNGAL потребують належного лікування з ретельним контролем артеріального тиску та виділення сечі, уживання відповідних доз діуретиків, щоб уникнути розвитку ГПН.
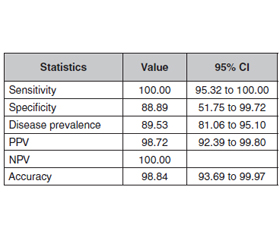
Background. The exact association between urinary neutrophil gelatinase-associated lipocalin (uNGAL) and acute kidney injury (AKI) is unknown in a critical care setting, in which the population is heterogeneous and the aetiology of AKI is unclear. Aim of this study is to clarify if uNGAL level is an early diagnostic marker for AKI in patients with sepsis. Materials and methods. The current study was conducted on 86 sepsis patients. The prevalence of AKI was identified among them. The role of uNGAL in predicting AKI development, mortality rate and length of the intensive care unit (ICU) stay were analyzed. Sensitivity and specificity were calculated, and the area under the receiver operating characteristic curve was considered as the optimal uNGAL cut-off level for detecting all classifications of AKI. Results. Most patients belonged to the age group of 51–60 years and their mean age was 54.6 years. Most patients (65.11 %) were males. 26.75 % had both type 2 diabetes mellitus and hypertension. AKI was detected in 89 % of subjects in the current study, as per KDIGO definition. 15.12 % of patients had stage 1 CKD, 15.12 % had stage 2 CKD, and stage 3 CKD was diagnosed in 4.65 % of cases. Mortality rate was 11 %, and 89 % of patients were discharged. The mean ICU length of stay among patients with AKI is 8.9 days. There is significant association between the mean ICU length of stay and AKI presence (p = 0.03). 17.4 % (n = 15) of patients required renal replacement therapy. There is a very significant difference in mean baseline uNGAL in patients with and without AKI: 149.9 and 73.2 ng/ml, respectively (p = 0.0006). This indicated that baseline uNGAL levels predict AKI. The mean uNGAL in people with AKI was 356 ng/ml and in those without AKI, it was 95 ng/ml. There is a very significant difference in mean uNGAL 48 hours after in patients with and without AKI (p < 0.0001). At a cut-off value of 120, there were 69 true positive cases, 9 true negative cases, 0 false positive cases, and 8 false negative cases. Based on these, the sensitivity of uNGAL at baseline in detecting AKI is 89.61 %, specificity is 100 %, and accuracy is 90.70 %. At a cut-off point of 120, there were 77 true positive cases, 8 true negative cases, 1 false positive case, and 0 false negative cases. Based on these, the sensitivity of uNGAL 48 hours after was 100 %, specificity 88.89 %, and accuracy was 98.84 %. There is a significant association between uNGAL levels and the ICU length of stay (p = 0.00). Conclusions. Sensitivity analysis was done in cut-off value of 120 for urinary NGAL in predicting AKI. From these results we conclude that urinary NGAL at the time of ICU admission is a reliable marker of renal function in sepsis patients. There is a significant correlation between AKI presence and urinary NGAL, and the ICU length of stay. We recommend not to use uNGAL alone in predicting AKI. It should be combined with glomerular filtration rate to reliably detect AKI development. Study findings indicate that sepsis patients with elevated uNGAL require proper management with close monitoring of blood pressure, urine output and appropriate doses of diuretics to avoid the development of AKI.
гостре ураження нирок; ліпокалін, асоційований iз желатиназою нейтрофілів, у сечі; специфічність; замісна ниркова терапія
acute kidney injury; urinary neutrophil gelatinase-associated lipocalin; specificity; renal replacement therapy
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Bonventre J.V., Zuk A. Ischemic acute renal failure: an inflammatory disease? Kidney Int. 2004. 66. 480-485. doi: 10.1111/j.1523-1755.2004.761_2.x.
- Schmidt-Ott K.M., Mori K., Kalandadze A., Li J.Y., Paragas N. et al. Neutrophil gelatinase-associated lipocalin-mediated iron traffic in kidney epithelia. Curr. Opin. Nephrol. Hypertens. 2006 Jul. 15(4). 442-9. doi: 10.1097/01.mnh.0000232886.81142.58.
- Cowland J.B., Borregaard N. Molecular characterization and pattern of tissue expression of the gene for neutrophil gelatinase-associated lipocalin from humans. Genomics. 1997. 45. 17-23. doi: 10.1006/geno.1997.4896.
- Carlson M., Raab Y., Seveus L., Xu S., Hallgren R., Venge P. Human neutrophil lipocalin is a unique marker of neutrophil inflammation in ulcerative colitis and proctitis. Gut. 2002. 50. 501-506. doi: 10.1136/gut.50.4.501.
- Mishra J., Dent C., Tarabishi R., Mitsnefes M.M., Ma Q. et al. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet. 2005. 365. 1231-1238. doi: 10.1016/S0140-6736(05)74811-X.
- Brunner H.I., Mueller M., Rutherford C., Passo M.H., Witte D. et al. Urinary neutrophil gelatinase-associated lipocalin as a biomarker of nephritis in childhood-onset systemic lupus erythematosus. Arthritis Rheum. 2006. 54. 2577-2584. doi: 10.1002/art.22008.
- Trachtman H., Christen E., Cnaan A., Patrick J., Mai V. et al., Investigators of the HUS-SYNSORB Pk Multicenter Clinical Trial. Urinary neutrophil gelatinase-associated lipocalcin in D+HUS: a novel marker of renal injury. Pediatr. Nephrol. 2006. 21. 989-994. doi: 10.1007/s00467-006-0146-y.
- Winther-Jensen M., Kjaergaard J., Lassen J.F., Køber L., Torp-Pedersen C. et al. Use of renal replacement therapy after out-of-hospital cardiac arrest in Denmark 2005–2013. Scand. Cardiovasc. J. 2018 Oct. 52(5). 238-243. doi: 10.1080/14017431.2018.1503707.
- Alobaidi R., Basu R.K., Goldstein S.L., Bagshaw S.M. Sepsis-associated acute kidney injury. Semin. Nephrol. 2015 Jan. 35(1). 2-11. doi: 10.1016/j.semnephrol.2015.01.002.
- Da Rocha E.P., Yokota L.G., Sampaio B.M., Cardoso Eid K.Z., Dias D.B. et al. Urinary Neutrophil Gelatinase-Associated Lipocalin Is Excellent Predictor of Acute Kidney Injury in Septic Elderly Patients.
- Aging Dis. 2018 Apr 1. 9(2). 182-191. doi: 10.14336/AD.2017.0307.
- Shyam R., Patel M.L., Kumar D., Sachan R., Chaudhary S.C., Gupta K.K. The prognostic value of neutrophil gelatinase-associated lipocalin in sepsis-associated acute kidney injury: a prospective observational study. Int. J. Crit. Illn. Inj. Sci. 2020 Sep. 10(Suppl. 1). 6-10. doi: 10.4103/IJCIIS.IJCIIS_80_19.
- Cao Y., Wang R.H. Associations among Metabolism, Circadian Rhythm and Age-Associated Diseases. Aging Dis. 2017 May 2. 8(3). 314-333. doi: 10.14336/AD.2016.1101.
- Mahajan S., Tiwar S., Bhowmik D., Agarwal S.K., Tiwari S.C., Dash S.C. Factors affecting the outcome of acute renal fai–lure among the elderly population in India: a hospital-based study. Int. Urol. Nephrol. 2006. 38. 391-6.
- Sesso R., Roque A., Vicioso B., Stella S. Prognosis of ARF in hospitalized elderly patients. Am. J. Kidney Dis. 2004 Sep. 44(3). 410-9.
- Kohli H.S., Bhat A., Aravindan, Sud K., Jha V. et al. Spectrum of renal failure in elderly patients. Int. Urol. Nephrol. 2006. 38(3–4). 759-65. doi: 10.1007/s11255-006-0089-z.
- Singbartl K., Kellum J.A. AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int. 2012 May. 81(9). 819-25. doi: 10.1038/ki.2011.339.
- Kim H., Hur M., Cruz D.N., Moon H.W., Yun Y.M. Plasma neutrophil gelatinase-associated lipocalin as a biomarker for acute kidney injury in critically ill patients with suspected sepsis. Clin. Biochem. 2013 Oct. 46(15). 1414-8. doi: 10.1016/j.clinbiochem.2013.05.069.
- Park H.S., Kim J.W., Lee K.R., Hong D.Y., Park S.O. et al. Urinary neutrophil gelatinase-associated lipocalin as a biomarker of acute kidney injury in sepsis patients in the emergency department. Clin. Chim. Acta. 2019 Aug. 495. 552-555. doi: 10.1016/j.cca.2019.06.005.
- Patel M.L., Sachan R., Shyam R., Kumar S., Kamal R., Misra A. Diagnostic accuracy of urinary neutrophil gelatinase-associated lipocalin in patients with septic acute kidney injury. Int. J. Nephrol. Renovasc. Dis. 2016 Jul 11. 9. 161-9. doi: 10.2147/IJNRD.S106781.
- Chronopoulos A., Rosner M.H., Cruz D.N., Ronco C. Acute kidney injury in elderly intensive care patients: a review. Intensive Care Med. 2010 Sep. 36(9). 1454-64. doi: 10.1007/s00134-010-1957-7.
- Collins A.J., Foley R.N., Chavers B., Gilbertson D., Herzog C. et al. US Renal Data System 2013 Annual Data Report. Am. J. Kidney Dis. 2014 Jan. 63(1 Suppl.). A7. doi: 10.1053/j.ajkd.2013.11.001.