
Архив офтальмологии Украины Том 12, №1, 2024
Вернуться к номеру
Дослідження показників внутрішньоочного тиску при різних видах тонометрії у пацієнтів з хворобою сухого ока
Авторы: Риков С.О., Пінчук Є.А.
Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
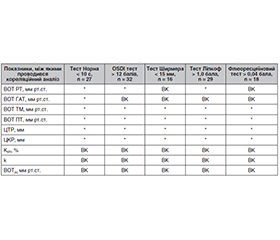
Актуальність. Протягом останнього часу глаукома залишається основною причиною необоротної сліпоти як у світі, так і в Україні. Підвищений внутрішньоочний тиск (ВОТ) залишається вирішальним фактором ризику розвитку глаукоми. Біомеханічні властивості рогівки потенційно можуть впливати на точність вимірювань ВОТ. Попередні дослідження показали, що зв’язок між центральною товщиною рогівки і ВОТ є нелінійним і може бути різним у рогівках нормальних очей і очей з хронічними захворюваннями. Метою нашого дослідження було вивчення показників внутрішньоочного тиску при різних видах тонометрії у пацієнтів з хворобою сухого ока. Матеріали та методи. 78 пацієнтів (78 правих очей) з еметропією та міопічною рефракцією слабкого ступеня взяли участь у дослідженні. Середній вік пацієнтів становив 23,8 ± 3,2 року. Серед обстежених було 36 чоловіків (46,15 %) і 42 жінки (53,85 %). До критеріїв виключення з дослідження належали: глаукома, цукровий діабет, гіпертонія, захворювання сполучної тканини, вагітність, дегенерація макули, дистрофія рогівки, рубець рогівки, набряк рогівки, кератоконус, хірургічні втручання на рогівці та оці, сферичний еквівалент (СЕ) ≥ 4,00 діоптрії, рогівковий астигматизм ≥ 3,00 діоптрії. Перед початком дослідження всі пацієнти підписали інформовану згоду на участь в ньому та були поінформовані про мету і хід дослідження. Протягом дослідження всі пацієнти проходили комплексне офтальмологічне обстеження. При визначенні ВОТ дотримувалися принципів рандомізації. Для визначення біомеханічних властивостей, коефіцієнта ригідності рогівки (KER) застосовували формули та спосіб оцінки ригідності рогової оболонки ока (Сергієнко М.М., Шаргородська І.В., 2008). Для кожного ока проводили розрахунок ВОТ з урахуванням коефіцієнта ригідності рогівки — ВОТ(к) та поправочного коефіцієнта з урахуванням коефіцієнта ригідності рогівки — k. Для статистичної обробки результатів дослідження застосовували програми Windows Microsoft Excel 2010, статистичне програмне забезпечення SPSS 17.0 (USA). Результати. Встановлено, що тест Норна в середньому по групі дорівнював 16,23 ± 10,20 с, при цьому 34,16 % учасників дослідження мали значення тесту Норна нижче від 10 с. Не визначалася статистично значуща різниця в значеннях тесту Норна між жінками та чоловіками (p = 0,518). Виявлено, що отриманий середній бал OSDI становив 10,54 ± 6,41 та у 41,02 % випадків середній бал OSDI перевищував 12 балів. Встановлені відмінності між жінками та чоловіками не було статистично значущі (p = 0,613). Крім того, аналіз результатів свідчив, що середні значення при визначенні ВОТ за допомогою різних тонометрів при зміні показників діагностичних проб і проявах сухого ока були завищені. Найменш уразливими були значення, отримані за допомогою апланаційної тонометрії Гольдмана. Неякісна слізна плівка має негативний оптичний вплив. Важливим результатом наших досліджень є те, що визначені за допомогою способу оцінки ригідності рогової оболонки ока (Сергієнко М.М., Шаргородська І.В., 2008) біомеханічні властивості рогівки не залежали від якості і кількості сльози та інших маркерів сухого ока. Не виявлено статистично значущої залежності між показником коефіцієнта ригідності рогівки, поправочним коефіцієнтом з урахуванням коефіцієнта ригідності рогівки та показниками тесту Норна (< 10 с), OSDI тесту (> 12 балів), тесту Ширмера (< 15 мм) та флюоресцеїнового тесту (> 0,04 балів). Значення ВОТ, коригованого на ригідність рогівки, статистично суттєво не відрізнялося між різними моделями. Висновки. Результати дослідження є свідченням того, що слізна плівка має вплив на параметри визначення внутрішньоочного тиску, виміряного за допомогою рикошетної тонометрії (РТ), апланаційної тонометрії Маклакова (ТМ) та пневмотонометрії (ПТ). Показано, що ВОТ, виміряний за допомогою РТ, ТМ та ПТ, має певну кореляцію з OSDI тестом і тестом Норна та кореляцію з тестом Ліпкоф і флюоресцеїновим тестом при ТМ та ПТ. Доведено відсутність залежності між показником коефіцієнта ригідності рогівки KER, поправочним коефіцієнтом k та ВОТ(к) зі змінами показників діагностичних проб. Потрібні подальші дослідження, щоб зрозуміти характер змін ригідності рогівки при виражених ступенях хвороби сухого ока, різних станах поверхні ока і в різних вікових групах.
Background. In recent years, glaucoma remains the main cause of irreversible blindness both in the world and in Ukraine. Increased intraocular pressure (IOP) remains a decisive risk factor for the development of glaucoma. Biomechanical properties of the cornea can potentially affect the accuracy of IOP measurements. Previous studies have shown that the relationship between central retinal thickness and IOP is non-linear and may be different in the corneas of normal eyes and eyes with chronic diseases. The purpose of our study was to investigate intraocular pressure indicators with different types of tonometry in patients with dry eye disease. Material and methods. Seventy-eight right eyes (78 patients) with emmetropia and mild myopic refraction were examined. The average age of patients was 23.8 ± 3.2 years. Among them, there were 36 men (46.15 %) and 42 women (53.85 %). Exclusion criteria: glaucoma, diabetes, hypertension, connective tissue disease, pregnancy, macular degeneration, corneal dystrophy, corneal scar, corneal edema, keratoconus, corneal and ocular surgery, spherical equivalent ≥ 4.00 diopter, corneal astigmatism ≥ 3.00 diopter. Before the start of the study, all patients signed informed consent to participate in it and were informed about the purpose and course. During the study, all patients underwent a comprehensive eye examination. When determining IOP, the principles of randomization were followed. In order to evaluate the biomechanical properties, the coefficient of corneal rigidity (KER), formulas and a method for assessing the corneal rigidity (Sergienko M.M., Shargorodska I.V., 2008) were used. For each eye, intraocular pressure was calculated taking into account the corneal rigidity coefficient — IOP(k) and the correction factor taking into account the corneal rigidity coefficient — k. Windows Microsoft Excel 2010, statistical software SPSS 17.0 (USA) were used for statistical processing of research results. Results. It was found that the non-invasive break-up time (NIBUT) was equal to 16.23 ± 10.20 seс on average for the group, while 34.16 % of the study participants had a NIBUT value below 10 sec. There was no statistically significant difference in NIBUT values between women and men (p = 0.518). It was found that the obtained average Ocular Surface Disease Index (OSDI) was 10.54 ± 6.41 points and in 41.02 % of cases, it exceeded 12 points. The detected differences between women and men were not statistically significant (p = 0.613). In addition, the analysis of the results showed that the average values of intraocular pressure measured using different tonometers with changes in the indicators of diagnostic tests and manifestations of dry eye were inflated. The least vulnerable were the values obtained using Goldmann applanation tonometry. A poor-quality tear film has a negative optical effect. An important result of our research is that the biomechanical properties of the cornea determined by the method for assessing the corneal rigidity (Sergienko M.M., Shargorodska I.V., 2008) did not depend on the quality and quantity of tears and other markers of dry eye. No statistically significant relationship was found between the corneal rigidity coefficient, the correction factor taking into account the corneal rigidity coefficient and NIBUT (< 10 s), OSDI (> 12 points), Schirmer’s test (< 15 mm) and fluorescein eye stain test (> 0.04 points). The value of IOP adjusted for corneal rigidity was not statistically significantly different between different models. Conclusions. The results of the study are evidence that the tear film influences the parameters of intraocular pressure measured by rebound tonometry (RT), Maklakov applanation tonometry (MAT) and pneumotonometry (PT). It has been shown that IOP measured by RT, MAT and PT has a certain relationship with OSDI and NIBUT, and a correlation with the LIPCOF and fluorescein eye stain test at MAT and PT. It was proved that there is no dependence between the coefficient of corneal rigidity KER, the correction factor k and IOP(k) and changes in the indicators of diagnostic tests. Further studies are needed to understand the nature of changes in corneal rigidity with severe degrees of dry eye disease, different conditions of the ocular surface, and in various age groups.
внутрішньоочний тиск; коефіцієнт ригідності рогівки; поправочний коефіцієнт k; тонометрія; хвороба сухого ока; рогівка
intraocular pressure; coefficient of corneal rigidity; correction factor k; tonometry; dry eye disease; cornea
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology. 2014;121:2081-2090. doi: 10.1016/j.ophtha. 2014.05.013.
- Sedaghat MR, Moghaddam HM, Yekta AA, Elsheikh A, Khabazkhoob M, Ambrósio JR, Maddah N, Danesh Z. Biomechanically-Corrected Intraocular Pressure Compared To Pressure Measured With Commonly Used Tonometers In Normal Subjects. Clinical Optometry. 2019;11:127-133. http://doi.org/10.2147/OPTO.S220776.
- Silva FD, Lira M. Intraocular pressure measurement: A review. Survey of Ophthalmology. 2022;67(5);1319-1331. DOI: 10.1016/j.survophthal. 2022.03.001.
- Machiele R, Motlagh M, Patel BC. Intraocular Pressure. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532237/.
- Tribble JR, Otmani A, Kokkali E, Lardner E, Morgan JE, Williams PA. Retinal Ganglion cell degeneration in a rat magnetic bead model of ocular hypertensive glaucoma. Trans Vis Sci Tech. 2021;10:21. doi: 10.1167/tvst.10.1.21.
- Nuyen B, Mansouri K. Fundamentals and Advances in Tonometry. Asia Pac J Ophthalmol (Phila). 2015 Mar-Apr;4(2):66-75. doi: 10.1097/APO.0000000000000118.
- Dogru M, Simsek C, Kojima T, Aketa N, Tsubota K, Shimazaki J. The impact of noncontact tonometry and icare rebound tonometry on tear stability and dry eye clinical practice. JCM. 2022;11:2819. doi: 10.3390/jcm11102819.
- King-Smith PE, Fink BA, Fogt N, Nichols KK, Hill RM, Wilson GS. The thickness of the human precorneal tear film: evidence from reflection spectra. Invest Ophthalmol Vis Sci. 2000;41:3348-3359. https://iovs.arvojournals.org/article.aspx?articleid = 2123231.
- Pflugfelder SC, Stern ME. Biological functions of tear film. Exp Eye Res. 2020;197. doi: 10.1016/j.exer.2020.108115.
- Zhou L, Zhao SZ, Koh SK, et al. In-depth analysis of the human tear proteome. J Proteomics. 2012;75:3877-3885. doi: 10.1016/j. jprot.2012.04.053.
- Yokoi N, Georgiev GA. Tear film-oriented diagnosis and tear film-oriented therapy for dry eye based on tear film dynamics. Invest Ophthalmol Vis Sci. 2018;59:DES13. doi: 10.1167/iovs.17-23700.
- Craig JP, Nichols K., Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15:276-283. doi: 10.1016/j.jtos. 2017.05.008.
- Papas EB. The global prevalence of dry eye disease: a Bayesian view. Ophthalmic Physiol Opt. 2021;41:1254-1266. doi: 10.1111/opo. 12888.
- Firat PG, Doganay S. Corneal hysteresis in patients with dry eye. Eye (Lond). 2011 Dec;25(12):1570-1574. doi: 10.1038/eye.2011.211.
- McMonnies CW. The significance of intraocular pressure elevation during sleep-related postures. Clin Exp Optom. 2014 May;97(3):221-4. doi: 10.1111/cxo.12108.
- Buey MA, Cristóbal JA, Ascaso FJ, Lavilla L, Lanchares E. Biomechanical Properties of the Cornea in Fuchs’ Corneal Dystrophy. Investigative Ophthalmology & Visual Science. 2009 July;50:3199-3202. doi: https://doi.org/10.1167/iovs.08-3312.
- Сергієнко М.М., Шаргородська І.В. Спосіб оцінки ригідності рогової оболонки ока. Патент на корисну модель 39262 Україна, МПК (2009) A61B 8/10.№а2008 02125; заявл. 19.02.2008; опубл. 25.02.2009, Бюл. № 4. C. 4.20.
- Шаргородська І.В. Роль біомеханічних властивостей фіброзної оболонки ока при аномаліях рефракції та кератоконусі: дис. … д-ра мед. наук. Київ, 2017. 403 с.
- Sergienko NM, Shargorodska IV. Determining corneal hysteresis and preexisting intraocular pressure. J Cataract Refract Surg. 2009;35:2033-2034.
- Maïssa C, Guillon M. Tear film dynamics and lipid layer characteristics — effect of age and gender. Contact Lens Anterior Eye. 2010;33:176-182. doi: 10.1016/j.clae.2010.02.003.
- Sherry A, Aridi M, Ghach W. Prevalence and risk factors of symptomatic dry eye disease in Lebanon. Contact Lens Anterior Eye. 2020;43:355-358. doi: 10.1016/j.clae.2019.08.001.
- Satitpitakul V, Taweekitikul P, Puangsricharern V, Kasetsuwan N, Reinprayoon U, Kittipibul T. Alteration of corneal biomechanical properties in patients with dry eye disease. PLoS One. 2021;16. doi: 10.1371/journal.pone.0254442.
- Long Q, Wang J, Yang X, Jin Y, Ai F, Li Y. Assessment of corneal biomechanical properties by CorVis ST in patients with dry eye and in healthy subjects. J Ophthalmol. 2015;2015:1-7. https://doi.org/10.1155 /2015/380624.
- Bao F, Huang Z, Huang J, et al. Clinical evaluation of methods to correct intraocular pressure measurements by the Goldmann applanation tonometer, ocular response analyzer, and Corvis ST tonometer for the effects of corneal stiffness parameters. J Glaucoma. 2016;25(6):510-519. doi: 10.1097/IJG. 0000000000000359.
- Bao F, Deng M, Wang Q, et al. Evaluation of the relationship of corneal biomechanical metrics with physical intraocular pressure and central corneal thickness in ex vivo rabbit eye globes. Exp Eye Res. 2015;137:11-17. doi: 10.1016/j.exer.2015.05.018.
- Doughty MJ, Zaman ML. Human corneal thickness and its impact on intraocular pressure measures: a review and meta-analysis approach. Surv Ophthalmol. 2000;44(5):367-408.
- Reznicek L, Muth D, Kampik A, Neubauer AS, Hirneiss C. Evaluation of a novel Scheimpflug-based non-contact tonometer in healthy subjects and patients with ocular hypertension and glaucoma. Br J Ophthalmol. 2013;97(11):1410-1414. doi: 10.1136/bjophthalmol-2013-303400.
- Salvetat ML, Zeppieri M, Tosoni C, Brusini P. Repeatability and accuracy of applanation resonance tonometry in healthy subjects and patients with glaucoma. Acta Ophthalmol. 2014;92(1):66-73. doi: 10.1111/aos.12209.
- Elsheikh A, Alhasso D, Gunvant P, Garway-Heath D. Multiparameter correction equation for Goldmann applanation tonometry. Optom Vis Sci. 2011;88(1):102-112. doi: 10.1097/OPX.0b013e3181fc3453.
- Huseynova T, Waring GO, Roberts C, Krueger RR, Tomita M. Corneal biomechanics as a function of intraocular pressure and pachymetry by dynamic infrared signal and Scheimpflug imaging ana–lysis in normal eyes. Am J Ophthalmol. 2014;157(4):885-893. doi: 10.1016/j.ajo.2013.12.024.
- Chui WS, Lam A, Chen D, Chiu R. The influence of corneal properties on rebound tonometry. Ophthalmology. 2008;115(1):80-84. doi: 10.1016/j.ophtha.2007.03.061.
- Suman S, Agrawal A, Pal VK, Pratap VB. Rebound tonometer: ideal tonometer for measurement of accurate intraocular pressure. J Glaucoma. 2014;23(9):633-637. doi: 10.1097/IJG.0b013e318285fefd.
- Pinero DP, Alcon N. In vivo characterization of corneal biomechanics. J Cataract Refract Surg. 2014;40(6):870-887. doi: 10.1016/j.jcrs.2014.03.021.
- Tonnu PA, Ho T, Newson T, et al. The influence of central corneal thickness and age on intraocular pressure measured by pneumotonometry, non-contact tonometry, the Tono-Pen XL, and Goldmann applanation tonometry. Br J Ophthalmol. 2005;89(7):851-854. doi: 10.1136/bjo.2004.056622.