
Журнал «Медицина неотложных состояний» Том 21, №2, 2025
Вернуться к номеру
Цільовий температурний контроль у поліпшенні церебрального метаболізму у пацієнтів з тяжкою черепно-мозковою травмою, асоційованою з розвитком гіпертермії
Авторы: Оленюк Д.В., Царьов О.В.
Дніпровський державний медичний університет, м. Дніпро, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
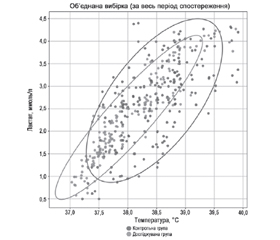
Актуальність. Тяжка черепно-мозкова травма (ЧМТ) залишається однією з основних причин смертності та інвалідизації працездатного населення. Запобігання вторинному пошкодженню мозку та його лікування є пріоритетною метою інтенсивної терапії. Тому контроль температури тіла та моніторинг церебрального метаболізму є значущими складовими інтенсивної терапії пацієнтів з ЧМТ. Мета: вивчити стан церебрального метаболізму у пацієнтів з тяжкою ЧМТ, асоційованою з розвитком гіпертермії центрального генезу, на підставі дослідження зв’язку між температурою ядра тіла та рівнем югулярного лактату при застосуванні цільового температурного контролю. Матеріали та методи. Досліджено 60 пацієнтів із тяжкою ЧМТ, асоційованою з розвитком гіпертермії, які перебували на лікуванні у відділенні інтенсивної терапії. Пацієнти були розподілені на дві групи: контрольна (n = 30) — зі стандартною антипіретичною терапією та досліджувана (n = 30) — із забезпеченням технології цільового температурного контролю за допомогою гіпотерма Blanketrol-II. Температура ядра тіла вимірювалася езофагеальним датчиком, рівень югулярного лактату визначався за допомогою біохімічного аналізатора. Статистичний аналіз проводився із застосуванням стандартних методів за допомогою Jupyter Notebook (https://jupyter.org). Результати. У першу добу дослідження медіана температури в обох групах перевищувала 38,3 °C і була вірогідно вищою в досліджуваній групі (p = 0,008). Починаючи з третьої доби у групі з контрольованою нормотермією медіанна температура була вірогідно (p < 0,001) нижчою — 37,8 °C. На сьому добу вона стабілізувалася в межах цільових значень, тоді як у контрольній групі температура залишалася підвищеною і була вірогідно вищою порівняно з досліджуваною групою (p = 0,005). Динаміка югулярного лактату демонструвала схожу тенденцію: вірогідно (p = 0,019) вищі показники в досліджуваній групі у першу добу дослідження, вірогідно (p = 0,004) нижчі медіанні рівні на третю добу у досліджуваній групі — 2,3 ммоль/л проти 3,2 ммоль/л у контрольній. Вірогідна (p < 0,001) різниця між групами при вищих рівнях у контрольній групі спостерігалася до шостої доби. Встановлено вірогідний (p < 0,001) сильний позитивний кореляційний зв’язок між температурою ядра тіла та рівнем югулярного лактату (rs = 0,83) при вірогідній (p < 0,001) різниці між групами: rs = 0,93 у досліджуваній групі порівняно з rs = 0,71 у контрольній. Висновки. Застосування технології цільового температурного контролю у пацієнтів з тяжкою ЧМТ, асоційованою з розвитком гіпертермії, сприяє ефективному зниженню температури тіла та підтриманню її в межах нормальних значень. А також зниженню порівняно з вихідними значеннями рівня югулярного лактату, що вказує на поліпшення церебрального метаболізму. Результати дослідження підтверджують необхідність впровадження методів температурного контролю в рутинну практику інтенсивної терапії тяжкої ЧМТ.
Background. Severe traumatic brain injury (TBI) remains one of the leading causes of mortality and disability among the working-age population. Preventing and treating secondary brain damage is a priority in intensive care. Therefore, temperature control and cerebral metabolism monitoring are essential components of intensive care for patients with severe TBI. Objective: to study the state of cerebral metabolism in patients with severe TBI associated with central hyperthermia by investigating the relationship between core body temperature and jugular lactate levels under targeted temperature control. Materials and methods. The study included 60 patients with severe TBI and associated hyperthermia who were treated in an intensive care unit. They were divided into two groups: the control one (n = 30) received standard antipyretic therapy, while the study group (n = 30) underwent targeted temperature control using the Blanketrol II hypothermia system. Core body temperature was measured using an esophageal probe, and jugular lactate levels were determined with a biochemical analyzer. Statistical analysis was conducted using standard methods in Jupyter Notebook (https://jupyter.org). Results. On the first day of the study, the median temperature in both groups exceeded 38.3 °C and was significantly higher in the study group (p = 0.008). From the third day, the median temperature in the controlled normothermia group was significantly lower (p < 0.001) at 37.8 °C. By the seventh day, it stabilized within target values, whereas in the control group, the temperature remained elevated and was significantly higher (p = 0.005). Jugular lactate dynamics had a similar trend: in the study group, significantly higher levels (p = 0.019) were observed on the first day, while on the third day, median levels were significantly lower — 2.3 mmol/L compared to 3.2 mmol/L in the control group (p = 0.004). A significant (p < 0.001) difference between groups persisted until the sixth day, with higher levels in the control group. There was a strong positive correlation (p < 0.001) between core body temperature and jugular lactate levels (rs = 0.83), with a significant (p < 0.001) difference between groups: rs = 0.93 in the study group vs. rs = 0.71 in the control one. Conclusions. The use of targeted temperature control technology in patients with severe TBI associated with hyperthermia allows for the effective reduction of body temperature and its maintenance within normal values, as well as a decrease in jugular lactate levels compared to baseline, which indicates an improvement in cerebral metabolism. The results of the study confirm the need to introduce temperature control methods into the routine practice of intensive care in severe TBI.
черепно-мозкова травма; цільовий температурний контроль; гіпертермія; лактат; церебральний метаболізм; інтенсивна терапія
traumatic brain injury; targeted temperature control; hyperthermia; lactate; cerebral metabolism; intensive care
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Maas AIR, Menon DK, Manley GT, et al. Traumatic brain injury: progress and challenges in prevention, clinical care, and research [published correction appears in Lancet Neurol. 2022 Dec;21(12):e10. doi: 10.1016/S1474-4422(22)00411-2]. Lancet Neurol. 2022;21(11):1004-1060. doi: 10.1016/S1474-4422(22)00309-X.
- Wiles MD. Management of traumatic brain injury: a narrative review of current evidence. Anaesthesia. 2022;77 Suppl 1:102-112. doi: 10.1111/anae.15608.
- Centers for Disease Control and Prevention: Moderate to Severe Traumatic Brain Injury is a Lifelong Condition; 2023. https://www.cdc.gov/traumaticbraininjury/pdf/moderate_to_severe_tbi_lifelong-a.pdf. Accessed Dec 2023.
- Menon DK, Schwab K, Wright DW, Maas AI; Demographics and Clinical Assessment Working Group of the International and Interagency Initiative toward Common Data Elements for Research on Traumatic Brain Injury and Psychological Health. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. 2010;91(11):1637-1640. doi: 10.1016/j.apmr.2010.05.017.
- Wu X, Tao Y, Marsons L, Dee P, Yu D, Guan Y, et al. The effectiveness of early prophylactic hypothermia in adult patients with traumatic brain injury: A systematic review and meta-analysis. Aust Crit Care. 2021;34(1):83-91. doi: 10.1016/j.aucc.2020.05.005.
- Bender M, Friedrich M, Voigtmann H, Haferkorn K, Uhl E, Stein M. Impact of Serum Lactate as an Early Serum Biomarker for Cardiopulmonary Parameters within the First 24 Hours of Intensive Care Unit Treatment in Patients with Isolated Traumatic Brain Injury. Diagnostics (Basel). 2023;13(10):1777. Published 2023 May 17. doi: 10.3390/diagnostics13101777.
- Lavinio A, Coles JP, Robba C, Aries M, Bouzat P, Chean D, et al. Targeted temperature control following traumatic brain injury: ESICM/NACCS best practice consensus recommendations. Crit Care. 2024;28(1):170. Published 2024 May 20. doi: 10.1186/s13054-024-04951-x.
- Hinson HE, Rowell S, Morris C, Lin AL, Schreiber MA. Early fever after trauma: Does it matter? J Trauma Acute Care Surg. 2018;84(1):19-24. doi: 10.1097/TA.0000000000001627.
- Andrews PJD, Verma V, Healy M, Lavinio A, Curtis C, Reddy U, et al. Targeted temperature management in patients with intracerebral haemorrhage, subarachnoid haemorrhage, or acute ischaemic stroke: consensus recommendations. Br J Anaesth. 2018;121(4):768-775. doi: 10.1016/j.bja.2018.06.018.
- Madden LK, Hill M, May TL, Human T, Guanci MM, Jacobi J, et al. The Implementation of Targeted Temperature Management: An Evidence-Based Guideline from the Neurocritical Care Society. Neurocrit Care. 2017;27(3):468-487. doi: 10.1007/s12028-017-0469-5.
- Hawryluk GWJ, Aguilera S, Buki A, Bulger E, Citerio G, Cooper DJ, et al. A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2019;45(12):1783-1794. doi: 10.1007/s00134-019-05805-9.
- Sharma B, Jiang W, Dhole Y, et al. Lactate Is a Strong Predictor of Poor Outcomes in Patients with Severe Traumatic Brain Injury. Biomedicines. 2024;12(12):2778. Published 2024 Dec 6. doi: 10.3390/biomedicines12122778.
- Stefani MA, Modkovski R, Hansel G, et al. Elevated glutamate and lactate predict brain death after severe head trauma. Ann Clin Transl Neurol. 2017;4(6):392-402. Published 2017 May 4. doi: 10.1002/acn3.416.
- Carpenter KL, Jalloh I, Hutchinson PJ. Glycolysis and the significance of lactate in traumatic brain injury. Front Neurosci. 2015;9:112. Published 2015 Apr 8. doi: 10.3389/fnins.2015.00112.
- Bakker J, Postelnicu R, Mukherjee V. Lactate: Where Are We Now? Crit Care Clin. 2020;36(1):115-124. doi: 10.1016/j.ccc.2019.08.009.
- Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate levels. Mayo Clin Proc. 2013;88(10):1127-1140. doi: 10.1016/j.mayocp.2013.06.012.
- Swan KL, Avard BJ, Keene T. The relationship between elevated prehospital point-of-care lactate measurements, intensive care unit admission, and mortality: A retrospective review of adult patients. Aust Crit Care. 2019;32(2):100-105. doi: 10.1016/j.aucc.2018.02.006.
- Martin-Rodriguez F, Sanz-Garcia A, Lopez-Izquierdo R, et al. Prehospital Lactate Levels Obtained in the Ambulance and Prediction of 2-Day In-Hospital Mortality in Patients with Traumatic Brain Injury. Neurology. 2024;103(4):e209692. doi: 10.1212/WNL.0000000000209692.