
Международный эндокринологический журнал Том 19, №1, 2023
Вернуться к номеру
Сімейна поведінкова терапія в лікуванні ожиріння в дітей шкільного віку
Авторы: T.V. Sorokman, S.V. Sokolnyk, N.O. Popeluk
Bukovinian State Medical University, Chernivtsi, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
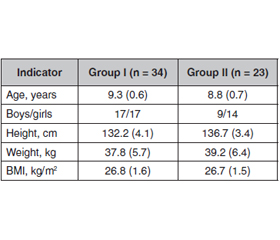
Актуальність. Ожиріння вражає 27–34 % дітей і вважається головною проблемою громадського здоров’я. Оскільки все більше дітей страждають від надмірної маси тіла, медичним працівникам необхідно шукати ефективні методи профілактики та лікування ожиріння. Мета: оцінити ефективність сімейної поведінкової терапії в лікуванні дітей із ожирінням. Матеріали та методи. Впродовж одного року під спостереженням перебувало 57 дітей віком 7–12 років з ожирінням, які були рандомізовані в дві групи: основну (інтервенційна) — 34 особи (I) та порівняння — 23 особи (II). Діти I групи включені в програму сімейного поведінкового лікування, що полягала в гіпокалорійному харчуванні, контролі за сімейним середовищем та дозованому контрольованому фізичному навантаженні. Ліпідний спектр крові вивчався за рівнем загального холестерину (ЗХС), тригліцеридів (ТГ), холестерину ліпопротеїнів низької (ХС ЛПНЩ) і високої щільності (ХС ЛПВЩ). Результати. У дітей з ожирінням як систолічний (САТ), так і діастолічний артеріальний тиск (ДАТ) був підвищений (становив у середньому 125,9 ± 0,9 мм рт.ст. i 66,9 ± 1,2 мм рт.ст. відповідно), також виявлено зростання концентрації ЗХС, ТГ, ХС ЛПНЩ. Через рік після проведення сімейної поведінкової терапії ІМТ у дітей з ожирінням знизився з 26,8 до 25,1 кг/м2, міжгрупові зміни САТ та ДАТ були статистично значущі (I група: до програми САТ становив 124,9 ± 0,8 мм рт.ст., після — 118,9 ± 0,9 мм рт.ст., р < 0,05; ДАТ — 65,7 ± 1,2 мм рт.ст. і 62,1 ± 1,0 мм рт.ст. відповідно, р < 0,05; II група: до програми САТ був 125,1 ± 0,7 мм рт.ст., після — 126,9 ± 0,8 мм рт.ст., р > 0,05; ДАТ — 66,6 ± 1,1 мм рт.ст. і 67,7 ± 1,2 мм рт.ст. відповідно, р > 0,05). Також відбулися достовірні зміни в ліпідному спектрі крові: рівень ЗХС знизився в 0,87 разa, ТГ — у 0,94 разa, при тенденції до зниження ХС ЛПНЩ та підвищення ХС ЛПВЩ. Висновки. Полікомпонентна сімейна поведінкова терапія є ефективною щодо зниження індексу маси тіла дітей з ожирінням. Отримані результати вказують на необхідність застосування запропонованої лікувальної програми в клінічній практиці.
Background. Obesity affects 27–34 % of children and is considered a major public health problem. As more and more children suffer from overweight, health professionals need to find effective methods of obesity prevention and treatment. The purpose was to evaluate the effectiveness of family behavioral therapy in the treatment of obese children. Materials and methods. For one year, 57 obese patients aged 7–12 years were under observation, they were randomly divided into 2 groups: a treatment group of 34 children (I) and a comparison group of 23 people (II). Group I children participated in the family behavioral treatment program, which included hypocaloric nutrition, control over the family environment, and dosed, controlled physical activity. The blood lipid spectrum was studied by the level of total cholesterol (TCh), triglycerides (TG), low-density lipoprotein cholesterol (LDL-Ch) and high-density lipoprotein cholesterol (HDL-Ch). Results. In obese children, both systolic (SBP) and diastolic blood pressure (DBP) were elevated (mean of 125.9 ± 0.9 mm Hg and 66.9 ± 1.2 mm Hg, respectively), an increase in the concentration of TCh, TG, and LDL-Ch was detected. One year after family behavioral therapy, body mass index in obese children decreased from 26.8 to 25.1 kg/m2, changes in SBP and DBP were statistically significant between groups (group I: SBP before was 124.9 ± 0.8 mm Hg, after — 118.9 ± 0.9 mm Hg, p < 0.05; DBP was 65.7 ± 1.2 mm Hg and 62.1 ± 1.0 mm Hg, respectively, p < 0.05; group II: SBP before the program was 125.1 ± 0.7 mm Hg, after — 126.9 ± 0.8 mm Hg, p > 0.05, DBP was 66.6 ± 1.1 mm Hg and 67.7 ± 1.2 mm Hg, respectively, p > 0.05), and there were also significant changes in blood lipids: the level of cholesterol decreased by 0.87 times, TG — by 0.94 times, with a tendency to LDL-Ch decrease and HDL-Ch increase. Conclusions. Multicomponent family behavioral therapy is effective in reducing the body mass index of obese children. The obtained results indicate the need to apply the proposed treatment program in clinical practice.
діти шкільного віку; ожиріння; індекс маси тіла; артеріальний тиск; ліпідний спектр; сімейна поведінкова терапія
school-aged children; obesity; body mass index; blood pressure; lipid spectrum; family behavioral treatment
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Di Cesare M., Sorić M., Bovet P., Miranda J.J., Bhutta Z. et al. The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action. BMC Med. 2019 Nov 25. 17(1). 212. doi: 10.1186/s12916-019-1449-8.
- Klingelhöfer D., Braun M., Quarcoo D., Brüggmann D., Groneberg D.A. Epidemiological Influences and Requirements of Global Childhood Obesity Research. Obes. Facts. 2021. 14(4). 382-396. doi: 10.1159/000516777.
- Mardali F., Naziri M., Sohouli M.H. et al. Predictors of central and general obesity in Iranian preschool children: which anthropometric indices can be used as screening tools? BMC Pediatrics. 2022. 22(1). 320. doi: 10.1186/s12887-022-03365-4.
- Fang K., Mu M., Liu K., He Y. Screen time and childhood overweight/obesity: a systematic review and meta-analysis. Child Care Health Dev. 2019 Sep. 45(5). 744-753. doi: 10.1111/cch.12701.
- Hales C.M., Carroll M.D., Fryar C.D., Ogden C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief. 2017 Oct. 288. 1-8.
- Chen J.L., Guedes C.M., Lung A.E. Smartphone-based healthy weight management intervention for Chinese American ado–lescents: short-term efficacy and factors associated with decreased weight. J. Adolesc. Health. 2019. 64(4). 443-9. doi: 10.1016/j.jadohealth.2018.08.022.
- Luca A.C., Curpan A.S., Braha E.E., Ţarcă E., Iordache A.C., Luca F.A., Adumitrachioaiei H. Increasing Trends in Obesity-Rela–ted Cardiovascular Risk Factors in Romanian Children and Adolescents-Retrospective Study. Healthcare (Basel). 2022 Dec 5. 10(12). 2452. doi: 10.3390/healthcare10122452.
- Chai L.K., Farletti R., Fathi L., Littlewood R. A Rapid Review of the Impact of Family-Based Digital Interventions for Obesity Prevention and Treatment on Obesity-Related Outcomes in Primary School-Aged Children. Nutrients. 2019. 14(22). 4837. doi: 10.3390/nu14224837.
- Aceves-Martins M., López-Cruzm L., García-Botello M., Gu–tier–rez-Gómez Y.Y., Moreno-García C.F. Interventions to Treat Obesity in Mexican Children and Adolescents: Systematic Review and Meta-Analysis. Nutrition Reviews. 2022. 80(3). 544-560. doi: 10.1093/nutrit/nuab041.
- Hoare J.K., Jebeile H., Garnett S.P., Lister N. Novel dietary interventions for adolescents with obesity: a narrative review. Pediatric Obesity. 2021. 16(9). e12798. doi: 10.1111/ijpo.12798.
- Epstein L.H., Schechtman K.B., Kilanowski C., Ramel M., Moursi N.A. et al. Implementing family-based behavioral treatment in the pediatric primary care setting: design of the PLAN study. Contemp. Clin. Trials. 2021 Oct. 109. 106497. doi: 10.1016/j.cct.2021.106497.
- Pankiv V. Features of prediabetes management in adolescents with excessive body weight and obesity. International Journal of Endocrinology (Ukraine). 2022. 18(8). 436-439. doi: 10.22141/2224-0721.18.8.2022.1222.
- Brown T., Moore T.H., Hooper L., Gao Y., Zayegh A., Ijaz S., Elwenspoek M. et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019 Jul 23. 7(7). CD001871. doi: 10.1002/14651858.CD001871.pub4.
- Bailey-Davis L., Moore A.M., Poulsen M.N., Dzewaltowski D.A., Cummings S., DeCriscio L.R., Hosterman J.F. et al. Comparing enhancements to well-child visits in the prevention of obesity: ENCIRCLE cluster-randomized controlled trial. BMC Public Health. 2022 Dec 26. 22(1). 2429. doi: 10.1186/s12889-022-14827-w.
- Li B., Gao S., Bao W., Li M. Effectiveness of lifestyle interventions for treatment of overweight/obesity among children in China: a systematic review and meta-analysis. Front. Endocrinol. (Lausanne). 2022 Oct 31. 13. 972954. doi: 10.3389/fendo.2022.972954.
- Falalyeyeva T., Mamula Y., Scarpellini E., Leshchenko I., Humeniuk A., Pankiv I., Kobyliak N. Probiotics and obesity associated disease: an extended view beyond traditional strains. Minerva Gastroenterol. (Torino). 2021 Dec. 67(4). 348-356. doi: 10.23736/S2724-5985.21.02909-0.
- Pereira A.R., Oliveira A. Dietary Interventions to Prevent Childhood Obesity: A Literature Review. Nutrients. 2021 Sep 28. 13(10). 3447. doi: 10.3390/nu13103447.
- Chrissini M.K., Panagiotakos D.B. Public health interventions tackling childhood obesity at European level: a literature review. Prev. Med. Rep. 2022 Nov 22. 30. 102068. doi: 10.1016/j.pmedr.2022.102068.
- Elinder L.S., Patterson E., Nyberg G., Norman Å. A Healthy School Start Plus for prevention of childhood overweight and obesity in disadvantaged areas through parental support in the school setting — study protocol for a parallel group cluster randomised trial. BMC Public Health. 2018. 18(1). 459. doi: 10.1186/s12889-018-5354-4.
- Adab P., Barrett T., Bhopal R. The West Midlands ActiVe lifestyle and healthy Eating in School children (WAVES) study: a cluster randomised controlled trial testing the clinical effectiveness and cost-effectiveness of a multifaceted obesity prevention intervention programme targeted at children aged 6–7 years. Health Technology Assessment (Winchester, England). 2018. 22(8). 1-608. doi: 10.3310/hta22080.
- Li B., Pallan M., Liu W.J., Hemming K. The CHIRPY DRAGON intervention in preventing obesity in Chinese primary-school-aged children: a cluster-randomised controlled trial. PLoS Medicine. 2018. 16(11). e1002971. doi: 10.1371/journal.pmed.1002971.
- Mazur A., Zachurzok A., Baran J. Childhood Obesity: Position Statement of Polish Society of Pediatrics, Polish Society for Pediatric Obesity, Polish Society of Pediatric Endocrinology and Diabetes, the College of Family Physicians in Poland and Polish Association for Study on Obesity. Nutrients. 2022. 14(18). 3806. doi: 10.3390/nu14183806.
- Wyszyńska J., Ring-Dimitriou S., Thivel D. Physical Activity in the Prevention of Childhood Obesity: The Position of the European Childhood Obesity Group and the European Academy of Pediatrics. Frontiers in Pediatrics. 2020. 8. 535705. doi: 10.3389/fped.2020.535705.
- Valerio G., Maffeis C., Saggese S. Diagnosis, treatment and prevention of pediatric obesity: consensus position statement of the Italian Society for Pediatric Endocrinology and Diabetology and the Italian Society of Pediatrics. Italian Journal of Pediatrics. 2020. 44(1). 88. doi: 10.1186/s13052-018-0525-6.
- Trandafir L.M., Dodi G., Frasinari O. Tackling Dyslipidemia in Obesity from a Nanotechnology Perspective. Nutrients. 2022. 14(18). 3774. doi: 10.3390/nu14183774.