
Международный эндокринологический журнал Том 19, №8, 2023
Вернуться к номеру
Стан еректильної функції у чоловіків, які перехворіли на COVID-19, через 6 місяців після одужання
Авторы: Лучицький Є.В., Лучицький В.Є., Зубкова Г.А., Рибальченко В.М., Складанна І.І.
ДУ «Інститут ендокринології та обміну речовин ім. В.П. Комісаренка НАМН України», м. Київ, Україна
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
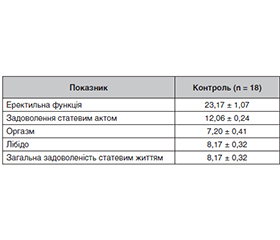
Актуальність. За результатами епідеміологічних досліджень встановлено, що COVID-19 частіше вражає чоловіків, ніж жінок. Серед ускладнень COVID-19 еректильна дисфункція розглядається як маркер ендотеліальної дисфункції та один з основних факторів розвитку серцево-судинних захворювань. Нижчі рівні загального та вільного тестостерону діють як провісники несприятливого прогнозу у чоловіків із SARS-CoV-2. Синдром дефіциту тестостерону розглядається як незалежний фактор ризику розвитку кардіометаболічних порушень. Мета роботи: дослідити стан еректильної функції у чоловіків, які перенесли COVID-19, через 6 місяців після одужання. Матеріали та методи. Обстежено 72 чоловіки, що хворіли на COVID-19, через 6,90 ± 0,29 місяця після одужання. Середній вік обстежених становив 45,23 ± 3,01 року. У контрольну групу включено 18 умовно здорових чоловіків віком 43,18 ± 2,90 року. Стан еректильної функції оцінювали за опитувальником «Міжнародний індекс еректильної функції» (МІЕФ). Концентрацію тестостерону визначали імуноферментним методом наборами фірми DRG (Німеччина), DiaMetra (Італія). Усі вимірювання проводили на аналізаторі Stat Fax 3200. Статистичний аналіз отриманих результатів між групами проводили за критерієм Стьюдента. Вірогідними вважали значення р < 0,05. Результати. Крім порушення еректильної функції, про що свідчить зниження відповідного інтегративного показника МІЕФ-15 «еректильна функція», у чоловіків, хворих на COVID-19, виявлено зниження статевого бажання, а також погіршення відчуттів у вигляді зменшення частоти сім’явивержень та оргастичних відчуттів під час статевих контактів. Середній рівень загального тестостерону в крові становив 10,9 нмоль/л та був вірогідно знижений порівняно з аналогічним показником у контрольній групі. Аналіз індивідуальних показників показав, що рівень тестостерону був знижений у 10 пацієнтів та був у межах нормальних значень у 13 чоловіків, хворих на COVID-19. Показник концентрації загального тестостерону в крові в обстежених чоловіків після перенесеного захворювання становив 10,73 ± 1,07 нмоль/л та був вірогідно знижений порівняно з показником контрольної групи. Висновки. Встановлено наявність еректильної дисфункції у чоловіків, які перехворіли на COVID-19, підтвердженої вірогідним зниженням показників МІЕФ-15 та інтегративних показників еректильної функції. В обстежених чоловіків встановлено вірогідне зниження концентрації загального тестостерону в крові, що може бути однією з причин еректильної дисфункції. Необхідні широкомасштабні проспективні рандомізовані контрольовані дослідження за участю пацієнтів, інфікованих SARS-CoV-2, щоб забезпечити розуміння молекулярних механізмів, які викликають порушення еректильної функції.
Background. Based on the results of epidemiological studies, it was found that coronavirus disease 2019 (COVID-19) affects men more often than women. Among COVID-19 complications, erectile dysfunction is considered a marker of endothelial dysfunction and one of the main factors for the development of cardiovascular diseases. Lower total and free testosterone levels are predictors of adverse prognosis in males with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Testosterone deficiency syndrome is considered an independent risk factor of cardiometabolic disorders. The purpose of the study is to investigate the state of erectile function in men who suffered from COVID-19 six months after recovery. Materials and methods. Seventy-two men suffering from COVID-19 and being treated in an infectious disease hospital were examined 6.90 ± 0.29 months after recovery. Their average age was 45.23 ± 3.01 years. The control group included 18 conditionally healthy men aged 43.18 ± 2.90 years. The state of erectile function was assessed using the International Index of Erectile Function (IIEF). The concentration of testosterone was determined by the enzyme-linked immunosorbent assay with DRG (Germany) and DiaMetra (Italy) kits. All measurements were performed on the Stat Fax 3200 analyzer. Statistical comparison of the obtained results between groups was performed according to the Student’s test. A value of p < 0.05 was considered to be significant. Results. In addition to erectile dysfunction, as evidenced by a reduced corresponding integrative indicator “erectile function” of IIEF-15 in men with COVID-19, a decrease in sexual desire was found, as well as a deterioration of sensations in the form of a decrease in ejaculation frequency and orgasmic sensations during sex contacts. The average serum level of total testosterone was 10.9 nmol/l and was significantly reduced compared to that in the control group. Analysis of individual indicators showed that testosterone level was decreased in 10 patients and was within the normal range in 13 men with COVID-19. The average serum concentration of total testosterone in the examined men after the disease was 10.73 ± 1.07 nmol/l and was significantly reduced compared to that of the control group. Conclusions. There was an erectile dysfunction in men who suffered COVID-19, it was confirmed by a probable decrease in IIEF-15 score and integrative indicators of erectile function. A significant decrease in the blood concentration of total testosterone was detected in the examined men, which may be one of the causes of erectile dysfunction. Large-scale prospective, randomized, controlled trials in patients infected with SARS-CoV-2 are needed to provide an understanding of the molecular mechanisms that cause erectile dysfunction.
еректильна дисфункція; COVID-19; опитувальник «Міжнародний індекс еректильної функції»; тестостерон
erectile dysfunction; COVID-19; International Index of Erectile Function; testosterone
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Pankiv V., Pashkovska N., Pankiv I., Maslyanko V., Tsaryk I. Pathophysiological and clinical aspects of interaction between coronavirus disease 2019 and thyroid. International Journal оf Endocrinology (Ukraine). 2021. 17(4). 329-333. https://doi.org/10.22141/2224-0721.17.4.2021.237348.
- Meng T.T., Dong R.J., Li T.G. Relationship between COVID-19 and the male reproductive system. Eur. Rev. Med. Pharmacol. Sci. 2021 Jan. 25(2). 1109-13. doi: 10.26355/eurrev_202101_24682. PMID: 33577068.
- Kresch E., Achua J., Saltzman R., Khodamoradi K., Aror H., Ibrahim E., et al. COVID-19 endothelial dysfunction can cause erectile dysfunction: histopathological, immunohistochemical, and ultrastructural study of the human penis. World J. Mens Health. 2021 Jul. 39(3). 466-469. doi: 10.5534/wjmh.210055.
- Fang D., Peng J., Liao S., Tang Y., Cui W., Yuan Y., et al. An online questionnaire survey on the sexual life and sexual function of Chinese adult men during the coronavirus disease 2019 Epidemic. Sex Med. 2021 Feb. 9(1). 100293. doi: 10.1016/j.esxm.2020.100293.
- Katz J., Yue S., Xue W., Gao H. Increased odds ratio for erectile dysfunction in COVID-19 patients. J. Endocrinol. Invest. 2022 Apr. 45(4). 859-64. doi: 10.1007/s40618-021-01717-y.
- Alonso-Domínguez J., Gallego-Rodríguez M., Martínez-Barros I., Calderón-Cruz B., Leiro-Fernández V., Pérez-González A. et al. High levels of IL-1β, TNF-α and MIP-1α one month after the onset of the acute SARS-CoV-2 infection, predictors of post COVID-19 in hospitalized patients. Microorganisms. 2023 Sep 26. 11(10). 2396. doi: 10.3390/microorganisms11102396.
- Guo T., Fan Y., Chen M., Wu X., Zhang L., He T., et al. Cardiovascular implications of fatal outcomes of patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020 Jul 1. 5(7). 811-8. doi: 10.1001/jamacardio.2020.1017. Erratum in: JAMA Cardiol. 2020 Jul 1. 5(7). 848.
- Hu B., Huang S., Yin L. The cytokine storm and COVID-19. J. Med. Virol. 2021 Jan. 93(1). 250-6. doi: 10.1002/jmv.26232.
- Sansone A., Mollaioli D., Ciocca G., Limoncin E., Colonnello E., Vena W., et al. Addressing male sexual and reproductive health in the wake of COVID-19 outbreak. J. Endocrinol. Invest. 2021 Feb. 44(2). 223-1. doi: 10.1007/s40618-020-01350-1.
- Harirugsakul K., Wainipitapong S., Phannajit J., Paitoonpong L., Tantiwongse K. Erectile dysfunction among Thai patients with COVID-19 infection. Transl. Androl. Urol. 2021 Dec. 10(12). 4376-83. doi: 10.21037/tau-21-807.
- Sardu C., Gambardella J., Morelli M.B., Wang X., Marfella R., Santulli G. Hypertension, thrombosis, kidney failure, and diabetes: Is COVID-19 an endothelial disease? A comprehensive evaluation of clinical and basic evidence. J. Clin. Med. 2020 May 11. 9(5). 1417. doi: 10.3390/jcm9051417.
- Pons S., Fodil S., Azoulay E., Zafrani L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Critical Care. 2020. 24(353). 1-8. doi.org/10.1186/s13054-020-03062-7.
- Duarte-Neto A.N., Teixeira T.A., Caldini E.G., Kanamura C.T., Gomes-Gouvêa M.S., Dos Santos A.B.G. et al. Testicular pathology in fatal COVID-19: A descriptive autopsy study. Andrology. 2022 Jan. 10(1). 13-23. doi: 10.1111/andr.13073.
- Dutta S., Sengupta P. SARS-CoV-2 and male infertility: Possible multifaceted pathology. Reprod. Sci. 2021 Jan. 28(1). 23-6. doi: 10.1007/s43032-020-00261-z.
- La Vignera S., Cannarella R., Condorelli R.A., Torre F., Aversa A., Calogero A.E. Sex-specific SARS-CoV-2 mortality: Among hormone-modulated ACE2 expression, risk of venous thromboembolism and hypovitaminosis D. Int. J. Mol. Sci. 2020 Apr 22. 21(8). 2948. doi: 10.3390/ijms21082948.
- Assyov Y., Gateva A., Karamfilova V., Gatev T., Nedeva I., Velikova T. et al. Impact of testosterone treatment on circulating irisin in men with late-onset hypogonadism and metabolic syndrome. Aging Male. 2020 Dec. 23(5). 1381-7. doi: 10.1080/13685538.2020.1770721.
- Dhindsa S., Zhang N., McPhaul M.J., Wu Z., Ghoshal A.K., Erlich E.C. et al. Association of circulating sex hormones with inflammation and disease sSeverity in patients with COVID-19. JAMA Netw Open. 2021 May 3. 4(5). e2111398. doi: 10.1001/jamanetworkopen.2021.11398.
- Cinislioglu A.E., Cinislioglu N., Demirdogen S.O., Sam E., Akkas F., Altay M.S. et al. The relationship of serum testosterone levels with the clinical course and prognosis of COVID-19 disease in male patients: A prospective study. Andrology. 2022 Jan. 10(1). 24-33. doi: 10.1111/andr.13081.
- Schroeder M., Tuku B., Jarczak D., Nierhaus A., Bai T., Jacobsen H. et al. The majority of male patients with COVID-19 present low testosterone levels on admission to Intensive Care in Hamburg, Germany: a retrospective cohort study. MedRxiv. 2020. 05.07.20073817. doi: https://doi.org/10.1101/2020.05.07.20073817.
- Gattinoni L., Chiumello D., Rossi S. COVID-19 pneumonia: ARDS or not? Crit. Care. 2020 Apr 16. 24(1). 154. doi: 10.1186/s13054-020-02880-z.
- Karsiyakali N., Sahin Y., Ates H.A., Okucu E., Karabay E. Evaluation of the sexual functioning of individuals living in Turkey during the COVID-19 pandemic: An internet-based nationwide survey study. Sex Med. 2021 Feb. 9(1). 100279. doi: 10.1016/j.esxm.2020.10.007.
- Costa T.J., Potje S.R., Fraga-Silva T.F.C., da Silva-Neto J.A., Barros P.R., Rodrigues D., et al. Mitochondrial DNA and TLR9 activation contribute to SARS-CoV-2-induced endothelial cell damage. Vascul. Pharmacol. 2022 Feb. 142. 106946. doi: 10.1016/j.vph.2021.106946.
- Fu J., Zhou B., Zhang L., Balaji K.S., Wei C., Liu X. et al. Expressions and significances of the angiotensin-converting enzyme 2 gene, the receptor of SARS-CoV-2 for COVID-19. Mol. Biol. Rep. 2020 Jun. 47(6). 4383-92. doi: 10.1007/s11033-020-05478-4.
- Li X., Chen Z., Geng J., Mei Q., Li H., Mao C. et al. COVID-19 and male reproduction: A thorny problem. Am. J. Mens Health. 2022 Jan-Feb. 16(1). 15579883221074816. doi: 10.1177/15579883221074816.
- Camici M., Zuppi P., Lorenzini P., Scarnecchia L., Pinnetti C., Cicalini S. et al. Role of testosterone in SARS-CoV-2 infection: A key pathogenic factor and a biomarker for severe pneumonia. Int. J. Infect. Dis. 2021 Jul. 108. 244-51. doi: 10.1016/j.ijid.2021.05.042.
- Lanser L., Burkert F.R., Thommes L., Egger A., Hoermann G., Kaser S. et al. Testosterone deficiency is a risk factor for severe COVID-19. Front. Endocrinol. (Lausanne). 2021 Jun 18. 12. 694083. doi: 10.3389/fendo.2021.694083.
- Salar R., Erbay G., Şanlı A., Yavuz U., Kandemir E., Turel H. et al. Effect of COVID-19 on the erectile function. Andrology. 2023 Jan. 11(1). 10-6. doi: 10.1111/andr.13315.