
Международный эндокринологический журнал Том 20, №1, 2024
Вернуться к номеру
Гострий інфаркт міокарда з елевацією сегмента ST у хворих на цукровий діабет 2-го типу. Вплив інгібітора НЗКТГ-2 дапагліфлозину
Авторы: M.I. Shved, I.O. Yastremska, V.Yu. Kuchmiy, R.M. Ovsiychuk
I. Horbachevsky Ternopil National Medical University, Ternopil, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
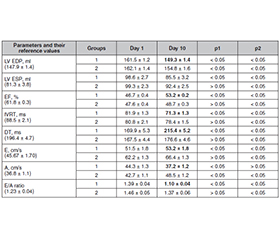
Актуальність. У пацієнтів із цукровим діабетом (ЦД) 2-го типу вдвічі вищий ризик розвитку ішемічної хвороби серця та смертності від неї, ніж в осіб без порушень вуглеводного обміну. Причиною таких негативних тенденцій вважають розвиток метаболічного стресу в умовах гіперглікемії та інсулінорезистентності, які лежать в основі порушення енергетичного метаболізму й ішемічного пошкодження кардіоміоцитів. Мета роботи: підвищити ефективність відновного лікування та оцінити динаміку показників якості життя у хворих із гострим коронарним синдромом (інфаркт міокарда з елевацією сегмента ST (STEMI)) на тлі ЦД 2-го типу та високим ризиком розвитку кардіальних ускладнень на стаціонарному етапі лікування шляхом включення в комплексну терапію інгібітора натрійзалежного котранспортера глюкози 2-го типу (НЗКТГ-2) дапагліфлозину. Матеріали та методи. Дослідну групу становили 38 хворих зі STEMI та ЦД 2-го типу, яким після черезшкірного коронарного втручання (ЧКВ) додатково призначали інгібітор НЗКТГ-2 дапагліфлозин. У контрольну групу увійшли 37 пацієнтів зі STEMI й ЦД 2-го типу, які після ЧКВ отримували лише стандартне протокольне лікування. Окрім загальноклінічних обстежень та оцінки якості життя за опитувальником EQ-5D-5L EuroQol Group (1990), проводили ехокардіографію з визначенням глобальної та локальної скорочувальної активності міокарда за методом Simpson, вивчали плазмові рівні глюкози, інсуліну, інсулінорезистентність — за індексом НОМА-IR. Результати. У хворих зі STEMI на тлі ЦД 2-го типу після коронарного втручання найчастіше розвивався реперфузійний синдром з проявами лівошлуночкової недостатності та порушень ритму. Під впливом стандартного медикаментозного лікування відзначалося суттєве клініко-функціональне покращення, але прогресувало післяінфарктне ремоделювання з порушенням систолічної та діастолічної функції і розвитком синдрому серцевої недостатності, також зберігалися резистентні до лікування пароксизми фібриляції передсердь, шлуночків, суправентрикулярні та шлуночкові екстрасистоли і блокади ніжок пучка Гіса. У хворих дослідної групи зі STEMI й ЦД 2-го типу на тлі комплексного медикаментозного лікування з включенням інгібітора НЗКТГ-2 дапагліфлозину відзначалося вірогідне зниження частоти порушень ритму і провідності вже на другу добу спостереження, а також зменшення ознак післяінфарктного ремоделювання лівого шлуночка, що в результаті проявлялося вірогідним покращенням скоротливості міокарда (фракція викиду зросла на 6,7 %) та зниженням діастолічної дисфункції. Також зареєстровано вірогідне зменшення частоти і вираженості реперфузійних аритмій, що досягнуто саме за рахунок кардіометаболічного впливу дапагліфлозину. Висновки. Включення в комплексне медикаментозне лікування інгібітора НЗКТГ-2 дапагліфлозину приводило до вірогідного покращення параметрів центральної кардіогемодинаміки та зниження частоти розвитку і вираженості реперфузійних аритмій та гострої лівошлуночкової недостатності, що сприяло покращенню показників якості життя.
Background. Patients with type 2 diabetes mellitus (T2DM) have a 2-fold higher risk of developing coronary heart disease and mortality than those without carbohydrate metabolism disturbances. The reason for such negative trends is the occurrence of metabolic stress due to hyperglycemia and insulin resistance, which causes disturbance in energy metabolism and ischemic damage to cardiomyocytes. The purpose of the study is to improve the effectiveness of rehabilitation treatment and assess the dynamics of quality of life in patients with ST-elevation myocardial infarction (STEMI) and T2DM who are at high risk of developing cardiac complications during the inpatient treatment by including the sodium-glucose transport protein 2 (SGLT2) inhibitor dapagliflozin in the comprehensive therapy. Materials and methods. The study group consisted of 38 patients with STEMI and T2DM who received dapagliflozin in addition to percutaneous coronary intervention (PCI). The control group included 37 patients with STEMI and T2DM who received only standard protocol treatment after PCI. In addition to general clinical examinations and assessment of quality of life using the EuroQol Group EQ-5D-5L questionnaire (1990), echocardiography was performed to determine general and local myocardial contractility by the Simpson method; plasma levels of glucose, insulin were evaluated, and insulin resistance was determined by the HOMA-IR. Results. Patients with STEMI and T2DM after PCI most often developed reperfusion syndrome with left ventricular failure and rhythm disturbances. Under the influence of standard medical treatment, a significant clinical and functional improvement was observed, but postinfarction remodeling progressed with impaired systolic and diastolic function and the development of heart failure syndrome, as well as treatment-resistant atrial and ventricular fibrillation paroxysms, supraventricular and ventricular extrasystoles, and bundle branch block. In patients of the study group with STEMI and T2DM on the comprehensive treatment with the SGLT2 inhibitor dapagliflozin, a significant decrease in the frequency of rhythm and conduction disturbances was noted on the second day of observation, as well as a decrease in postinfarction left ventricular remodeling, which ultimately manifested in a statistically significant improvement of myocardial contractility (ejection fraction increased by 6.7 %) and a decrease in diastolic dysfunction. There was also a significant decrease in the frequency and severity of reperfusion arrhythmias, which was achieved due to the cardiometabolic effect of the SGLT2 inhibitor dapagliflozin. Conclusions. The inclusion of the SGLT2 inhibitor dapagliflozin in the comprehensive treatment led to a significant improvement in central cardiac hemodynamic parameters and a decrease in the frequency and severity of reperfusion arrhythmias and acute left ventricular failure, which contributed to the improvement in quality of life.
цукровий діабет 2-го типу; інфаркт міокарда з елевацією сегмента ST; черезшкірне коронарне втручання; дапагліфлозин; якість життя
type 2 diabetes mellitus; ST-elevation myocardial infarction; percutaneous coronary intervention; dapagliflozin; quality of life
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Oksak G.A., Golovanova I.A. Contribution of mortality from cardiovascular disease to overall mortality. Wiad. Lek. 2017. 70(3, pt 1). 449-455.
- Ralapanawa U., Sivakanesan R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J. Epidemiol. Glob. Health. 2021 Jun. 11(2). 169-177. doi: 10.2991/jegh.k.201217.001.
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018 Nov 10. 392(10159). 1789-1858. doi: 10.1016/S0140-6736(18)32279-7.
- Pandey A., Wells C.R., Stadnytskyi V., Moghadas S.M., Marathe M.V. et al. Disease burden among Ukrainians forcibly displaced by the 2022 Russian invasion. Proc. Natl Acad. Sci. USA. 2023 Feb 21. 120(8). e2215424120. doi: 10.1073/pnas.2215424120.
- Megaly M., Schmidt C.W., Dworak M.W., Garberich R., Stanberry L. et al. Diabetic Patients Who Present with ST-Elevation Myocardial Infarction. Cardiovasc. Revasc. Med. 2022 May. 38. 89-93. doi: 10.1016/j.carrev.2021.08.003.
- Khan M.A.B., Hashim M.J., King J.K., Govender R.D., Mustafa H., Al Kaabi J. Epidemiology of Type 2 Diabetes — Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health. 2020 Mar. 10(1). 107-111. doi: 10.2991/jegh.k.191028.001.
- Daryabor G., Atashzar M.R., Kabelitz D., Meri S., Kalantar K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020 Jul 22. 11. 1582. doi: 10.3389/fimmu.2020.01582.
- Galicia-Garcia U., Benito-Vicente A., Jebari S., Larrea-Sebal A., Siddiqi H. et al. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020 Aug 30. 21(17). 6275. doi: 10.3390/ijms21176275.
- Anand S.S., Dagenais G.R., Mohan V., Diaz R., Probstfield J. et al.; EpiDREAM Investigators. Glucose levels are associated with cardiovascular disease and death in an international cohort of normal glycaemic and dysglycaemic men and women: the EpiDREAM cohort study. Eur. J. Prev. Cardiol. 2012 Aug. 19(4). 755-64. doi: 10.1177/1741826711409327.
- Einarson T.R., Acs A., Ludwig C., Panton U.H. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018 Jun 8. 17(1). 83. doi: 10.1186/s12933-018-0728-6.
- Damaskos C., Garmpis N., Kollia P., Mitsiopoulos G., Barlampa D. et al. Assessing Cardiovascular Risk in Patients with Diabetes: An Update. Curr. Cardiol. Rev. 2020. 16(4). 266-274. doi: 10.2174/1573403X15666191111123622.
- Ismail L., Materwala H., Al Kaabi J. Association of risk factors with type 2 diabetes: A systematic review. Comput. Struct. Biotechnol. J. 2021 Mar 10. 19. 1759-1785. doi: 10.1016/j.csbj.2021.03.003.
- Saeedi P., Salpea P., Karuranga S., Petersohn I., Malanda B. et al. Mortality attributable to diabetes in 20–79 year old adults, 2019 estimates: Results from the International Diabetes Federation Diabetes Atlas, 9th ed. Diabetes Res. Clin. Pract. 2020 Apr. 162. 108086. doi: 10.1016/j.diabres.2020.108086.
- Linkeviciute-Ulinskiene D., Kaceniene A., Dulskas A., Patasius A., Zabuliene L., Smailyte G. Increased Mortality Risk in People with Type 2 Diabetes Mellitus in Lithuania. Int. J. Environ. Res. Public Health. 2020 Sep 20. 17(18). 6870. doi: 10.3390/ijerph17186870.
- Chen Z., Ding S., Yuan Y., Du J., Zhang L. Relationship between Perioperative Cardiovascular Events and Glycated Hemoglobin in Diabetic Patients Undergoing Noncardiac Surgery. Biomed. Res. Int. 2020 Dec 17. 2020. 3645374. doi: 10.1155/2020/3645374.
- Zheng J., Cheng J., Wang T., Zhang Q., Xiao X. Does HbA1c Level Have Clinical Implications in Diabetic Patients Undergoing Coronary Artery Bypass Grafting? A Systematic Review and Meta-Analysis. Int. J. Endocrinol. 2017. 2017. 1537213. doi: 10.1155/2017/1537213.
- McMurray J.J.V., Solomon S.D., Inzucchi S.E., Køber L., Kosiborod M.N. et al.; DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019 Nov 21. 381(21). 1995-2008. doi: 10.1056/NEJMoa1911303.
- Nessler J. Dapagliflozin in the treatment of patients with heart failure with reduced left ventricular ejection fraction — a practical approach. Postepy Kardiol. Interwencyjnej. 2021 Jun. 17(2). 135-140. doi: 10.5114/aic.2021.107491.
- Bhatt D.L., Lopes R.D., Harrington R.A. Diagnosis and Treatment of Acute Coronary Syndromes: A Review. JAMA. 2022 Feb 15. 327(7). 662-675. doi: 10.1001/jama.2022.0358.
- Ibanez B., James S., Agewall S., Antunes M.J., Bucciarelli-Ducci C. et al.; ESC Scientific Document Group. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018 Jan 7. 39(2). 119-177. doi: 10.1093/eurheartj/ehx393.
- Rabin R., de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann. Med. 2001 Jul. 33(5). 337-43. doi: 10.3109/07853890109002087.
- Gyldenkerne C., Mortensen M.B., Kahlert J., Thrane P.G., Warnakula Olesen K.K. et al. 10-Year Cardiovascular Risk in Patients with Newly Diagnosed Type 2 Diabetes Mellitus. J. Am. Coll. Cardiol. 2023 Oct 17. 82(16). 1583-1594. doi: 10.1016/j.jacc.2023.08.015.
- Kosmas C.E., Bousvarou M.D., Kostara C.E., Papakonstantinou E.J., Salamou E., Guzman E. Insulin resistance and cardiovascular disease. J. Int. Med. Res. 2023 Mar. 51(3). 3000605231164548. doi: 10.1177/03000605231164548.
- Martín-Timón I., Sevillano-Collantes C., Segura-Galindo A., Del Cañizo-Gómez F.J. Type 2 diabetes and cardiovascular disease: Do all risk factors have the same strength? World J. Diabetes. 2014 Aug 15. 5(4). 444-70. doi: 10.4239/wjd.v5.i4.444.
- Pankiv V., Yuzvenko T. The relationships between variab–les of glycated hemoglobin and diabetes distress in patients with type 1 and type 2 diabetes mellitus. International Journal of Endocrinology (Ukraine). 2023. 19(6). 424-427. doi: 10.22141/2224-0721.19.6.2023.1310.
- Mao L., Cai D., Chi B., Xiao T., Zou A. et al. Dapagliflozin reduces the risk of heart failure rehospitalisation in diabetic acute myocardial infarction patients: a propensity score-matched analysis. Eur. J. Clin. Pharmacol. 2023 Jul. 79(7). 915-926. doi: 10.1007/s00228-023-03495-3.